Playlist
Show Playlist
Hide Playlist
Cerebral Toxoplasmosis, Neurocysticercosis and Parasitic Meningoencephalitis

-
Slides 10 CNSInfections Neuropathology I.pdf
-
Download Lecture Overview
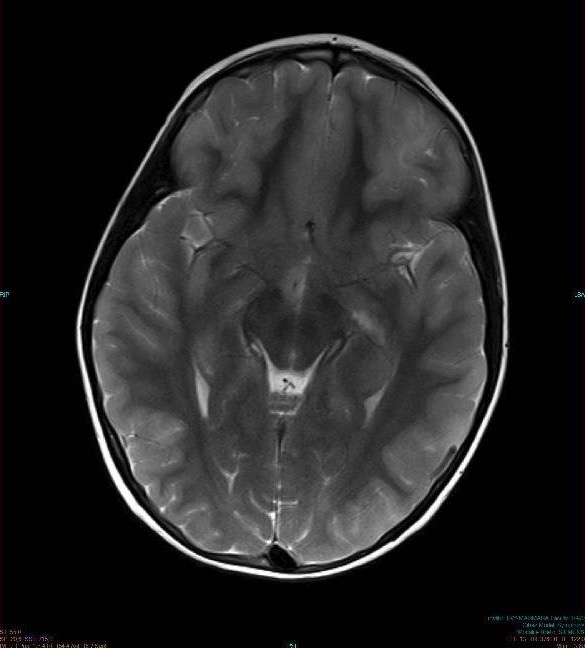
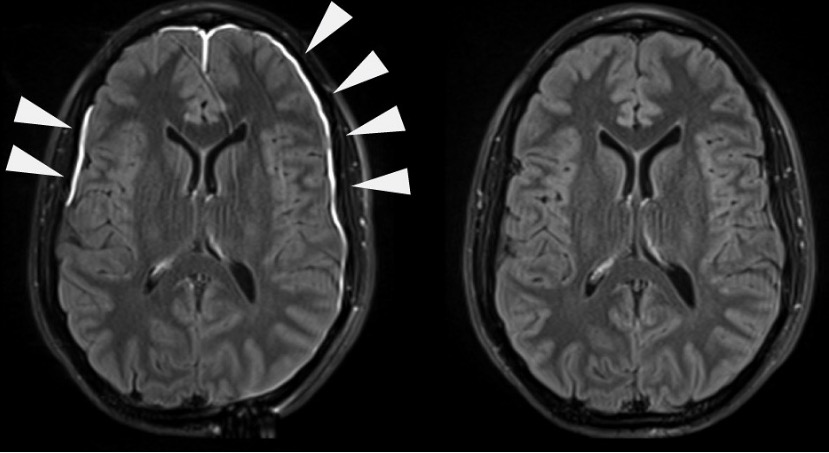
00:01 So let’s talk about that one parasitic known as cerebral toxoplasmosis. 00:06 First and foremost, who's your patient? A greater importance once again in AIDS epidemic unfortunately and the organism, gondii, Toxoplasma gondii, is one of the most common causes of neurologic symptoms in AIDS patients. 00:25 What is CT or MRI going to show you? You should know a list of differentials that will give you ring-enhanced lesions. 00:37 We’ll talk about brain abscess coming up. 00:39 Toxoplasma will give you ring-enhanced lesion. 00:43 What does that mean? I’ll show you a picture later, whereupon CT, you find this ring around the brain parenchyma. 00:51 You could have toxoplasma. 00:53 It could be brain abscess. 00:55 Later on, we’ll talk about gliobastoma multiforme, but that is a heterogeneous type of ring-enhanced lesion. 01:02 At this point, we’ll go with the basics. 01:05 Ring-enhanced lesion is a very important point or description or finding for further differentials and pathology. 01:12 A similar findings with CNS lymphoma, tuberculosis, or fungal infection. 01:17 Toxo. 01:19 There is a trial of toxo therapy if necessary. 01:21 Toxo is the most common cause of cerebral mass lesion in patients with AIDS. 01:27 So as soon as you hear about AIDS and you see a ring-enhanced lesion upon imaging, you should be thinking about toxo. 01:35 If you take a look at this particular imaging, what do you find? A ring-enhanced lesion. 01:42 You find a ring-enhanced lesion such as this apart from toxoplasmosis. 01:47 You should be thinking about abscess formation. 01:49 You see that, right there? Perfectly, perfectly ring-like structure. 01:55 If this patient has a CD4 count less than 50 and AIDS, in fact, has unfortunately settled in, most likely toxoplasmosis. 02:06 In laboratory workup, what are you going to do? CSF findings, if negative, a trial of therapy may still be attempted though. 02:14 Okay. So once again, can send serum and CSF serology, but if negative, still if you know your patient has AIDS, you still do empiric type of therapy. 02:26 Treatment, avoid steroids. 02:28 It actually hampers differential diagnosis. 02:31 Your pyrimethamine, sulfadiazine or folinic acid. 02:35 Life-long maintenance is required here if patient most likely immunocompromised. 02:43 Another type of parasitic infection here, apart from toxoplasmosis, would be neurocysticercosis. 02:50 This is a tapeworm and this is your soul pig. 02:54 "I’m sorry what?" Take a look Taenia solium and think of this pig, pork is what you should be thinking, right? And I’ll go ahead and call this soul pig if that helps you. 03:05 There are different types of Taenia. 03:07 At least know solium, please. 03:09 The most common parasitic infection of the CNS worldwide. 03:13 Look at this, not necessarily, immunocompromised really for the first time in a long time. 03:20 We talked about Cryptococcus, meningoencephalitis and that was immunocompromised. 03:24 We did toxoplasmosis. 03:26 That patient was immunocompromised. 03:28 Here, we have neurocysticercosis. 03:31 Most common parasitic infection of CNS worldwide. 03:34 Notice, we do not have an immunocompromised patient. 03:38 Are we clear? Endemic in Mexico and Central America. 03:43 Brain involvement in 50-70% of your cases. 03:47 Let’s talk about the clinical presentation of neurocysticercosis. 03:51 I’m going to bring in a couple of integration points here. 03:55 Seizures. 03:58 Headaches due to increased intracranial pressure. 04:00 So worldwide, most common parasitic CNS infection, right? And your patient is exposed to what organism? Taenia solium. 04:12 And what was I being silly about? Pork. 04:17 What’s interesting is that you might then form -- Take a look at the middle portion of this name. 04:23 Neuro-, cyst-, -cercosis. 04:28 What if this cyst ruptures in the brain? Now, what do we call this technically? Good. 04:35 Whenever you have a cyst that ruptures, you call this separately “chemical meningitis”. 04:42 Is that clear? The last time we saw a cyst that were rupturing is when we talked about dermoid tumor or for that matter any type of cyst that may rupture. 04:52 Here, exactly the same thing. 04:55 With neurocysticercosis, here is an imaging and an arrow particularly pointing to that cyst-like structure. 05:03 "Dr. Raj, how can I tell that this is a cyst and not a ring-like structure?" This is a ring enhancing cystic lesion. 05:10 As you can see the outer ring lit up surrounding a slightly more radiolucent central structure. 05:17 This indicates an active cyst as would be seen in neurocysticercosis. 05:23 With neuroimaging, I want you to be really careful with this statement. 05:27 Now, the ring enhancing cystic lesion, we have an active cyst. 05:32 Remember in the middle, you're going to be completely, well for the most part, it would be filled with fluid, it'd be a cyst. 05:41 The parenchymal calcification, even older cyst, and the vasogenic edema. 05:45 Now, this is quite interesting here and you want to pay attention in the detail here. 05:50 Why do you want to know so much detail about this? Because it is the most common parasitic sinus infection worldwide. 05:56 Okay. And you don't have to be immunocompromised. 06:01 So if it's an active lesion, and there's a cyst, granted, maybe it's ring enhancing, okay. 06:06 But more commonly, the presentation, the picture that I gave you earlier that imaging study, if you took a look at the middle, it wasn't transparent, right? It was not loosened. And so therefore, it was calcified. 06:21 Most commonly, that is a presentation that you might be given. 06:24 But just to be technical, yes, it could be bring enhance if with an active cyst, but usually by the time the patient is going to present, you're going to find that the cyst has now become calcified, which means that you have a very, very opaque structure. 06:39 Is that clear? And finally, the type of edema will be vasogenic. 06:43 What does that mean to you? It means that this is an inflammatory process. 06:47 And if it's an inflammatory process vasodilation and you edema have released a fluid or escape of fluid from your blood vessels resulting in what's known as vasogenic edema. 07:01 In the cerebral spinal fluid, usually normal and may show mononuclear pleocytosis, maybe mild increase in protein, but there is enough information here without CSF analysis to know that you're dealing with neurocysticercosis. 07:18 Treatment: Seizures with antiepileptics that is important. 07:23 What does this seizure mean to you? We know for a fact that the cause of seizures in neurocysticercosis is related to neuroinflammation and the release of P substance and not the space occupying nature of the lesion. 07:37 You should remember that these lesions are usually quite small. 07:42 When you think of cyst is? A space occupying lesion may then result in seizures. 07:47 Yeah, albendazole, it kill the parasite. 07:50 And steroids to maybe control the inflammation. 07:54 Continuing our discussion of infectious type of CNS. 07:59 We have more common in immunocompromised patients but this time we're parasitic. 08:04 Under these, we have toxoplasma. We'll talk about cysticercosis. 08:09 There's malaria, amebiasis, and also trypanosomiasis. 08:14 You've heard of trypanosoma before, in reference to Trypanosoma cruzi and Chaga. 08:20 We'll talk about toxo, talk about cysticercosis. 08:23 Parasitic meningoencephalitis. 08:26 More commonly, once again found in immunocompromised. 08:29 We have now, all I've talked about so far just fungal and cryptococcal that's where your focus should be on. 08:35 Now, we moved on to parasitic.
About the Lecture
The lecture Cerebral Toxoplasmosis, Neurocysticercosis and Parasitic Meningoencephalitis by Carlo Raj, MD is from the course CNS Infections - Clinical Neurology. It contains the following chapters:
- Cerebral Toxoplasmosis
- Neurocysticercosis
- Parasitic Meningoencephalitis
Included Quiz Questions
Which of the following is an unlikely cause of multiple ring-enhancing lesions in a CT or MRI of the head?
- Intracerebral hemorrhage
- Brain abscess
- Cerebral toxoplasmosis
- Glioblastoma multiforme
- CNS lymphoma
A 45-year-old Caucasian man with a history of HIV is brought to the ER after an episode of seizures. He has a history of alcoholism. There is no history of fever, chest pain, shortness of breath, nausea, vomiting, diarrhea, or constipation. Multiple ring-enhancing lesions are seen on his head CT. What is the next best step in the management of this patient?
- Trial of toxo therapy
- Trial of steroids
- Trial of antibiotics
- Trial of INH
- Trial of rifampicin
A 28 year-old incarcerated man presents to your office with fatigue and loss of weight. His CD4 count is 75 cells/mm3 and he has an HIV viral load of 100,000 copies/ml. His BMI is 18 kg/m2. His medical condition makes him highly susceptible to invasion from which parasite?
- Toxoplasma gondii
- Histoplasmosis
- Tuberculosis
- Treponema pallidum
- Cryptococcus
What is the most common CNS parasitic infection worldwide?
- Taenia solium
- Toxoplasma gondii
- Histoplasma capsulatum
- Cryptococcus neoformans
- Ascaris lumbricoides
Which of the following is NOT true about neurocysticercosis?
- Inhalation of spores from pigeon excreta
- Hydrocephalus due to rupture of an intraventricular cyst
- Chemical meningitis due to rupture of an intraventricular cyst
- Old cysts due to parenchymal calcification
- Mild mononuclear pleocytosis on CSF
Which of the following is the most common cause of intracerebral mass lesions in a patient with AIDS?
- Toxoplasmosis gondii
- Cryptococcus neoformans
- Taenia solium
- Histoplasma capsulatum
- Ascaris lumbricoides
Author of lecture Cerebral Toxoplasmosis, Neurocysticercosis and Parasitic Meningoencephalitis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
