Playlist
Show Playlist
Hide Playlist
Anatomy of the Breast

-
Slides Anatomy of the Breast.pdf
-
Download Lecture Overview
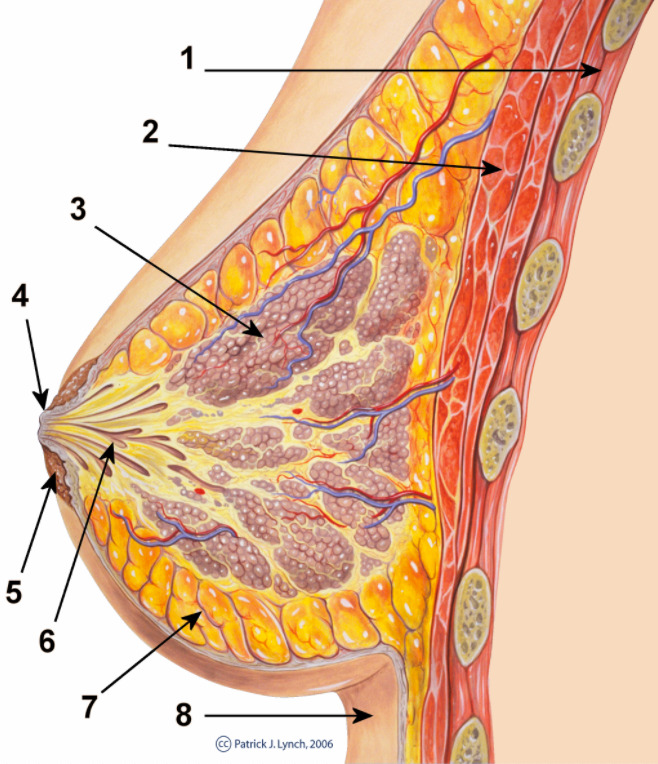
00:01 Now, we're going to talk about the breast. 00:04 The breast is where we have the mammary glands. 00:07 And the mammary glands are basically sweat glands that have been modified to form a milk for the nourishment of the young of mammal species such as humans. 00:17 In fact, "mamma" in Latin actually means breast, which is how mammals got their name. 00:22 The first thing we'll talk about when we talk about the breast is its overall shape and location. 00:28 And the first thing to get that down is this large muscle here, the pectoralis major. 00:34 And we're pointing that out because the majority of the breast essentially sits between the overlying skin and the fascia of the pectoralis deep to it. 00:44 The next thing we're going to point out, are the nipple and areola, not just because they represent the superficial termination of these ducts of these glands in the breast, but they also serve as an important central focus point when we talk about quadrants of the breast. 01:04 So, what do we mean by quadrants? So, when we talk about lesions or nodules in the breast, sometimes we want to have shorthand to get into the general area that we're talking about. 01:15 And so using the nipple as a center point, we divide the breast into quadrants very commonly, where we have an upper inner quadrant, a lower inner quadrant, a lower outer quadrant, and an upper outer quadrant. 01:31 Now, you'll also sometimes hear something called an axillary tail. 01:36 Axilla is our fancy word for armpit. 01:40 And sometimes axillary tail is thought of as a continuation of the upper outer quadrant. 01:47 And sometimes it can be but a lot of the time, it's actually not even connected to the upper outer quadrant, but it's actually disconnected and may represent some accessory breast tissue, which you can actually find anywhere from the axilla through the breast down to the groin, and a line called the milk line. 02:06 If we look at a sagittal cross section of the breast, we can see that the functional tissue of the breast is broken up into lobules that will feed into like different ducts that will eventually open up at the nipple. 02:21 In between these lobules and ducts are connective tissue that goes from the overlying epidermis down to the fascia deep to the breast. 02:32 Those are called suspensory ligaments. 02:35 However, the majority of the volume of the breast is made up of fat tissue. 02:41 When we talk about blood supply, probably won't surprise you. 02:44 We already mentioned the term axilla that we're going to see the axillary artery and that's going to be a major supplier of blood to the breast. 02:53 So the axillary artery has a few parts to it that you may have learned in the upper limb. 02:58 But we'll talk about those again here. 03:00 The first part has one artery called the superior thoracic, and the second part has too the thoracoacromial and the lateral thoracic arteries. 03:11 Another important artery for the breast is one we've already mentioned before the internal thoracic or internal mammary artery. 03:19 Now you can see why we use both terms. 03:22 You can see why mammary is an appropriate name because there is these branches that can supply the medial portion of the breast. 03:29 Finally, deep to the breast, we can get some good blood supply from those intercostal arteries, particularly the ones around the intercostal space 2 through 6. 03:42 As is the case in most of the body, the venous drainage mirrors the blood supply that comes anteriorly. 03:48 So we have the axillary vein, internal thoracic vein, and again, the intercostal veins, again of ribs 2 to 6. 04:00 Again, very similarly, the innervation is largely going to come from the underlying intercostal nerves from the ribs two through six. 04:11 Now, a bit more complicated is the lymphatic drainage, but it's very clinically relevant because there's a very high prevalence of breast cancer and knowing if cancer has reached the nodes that are being drained by these lymphatics here is an important part in breast cancer staging. 04:32 So we're going to spend some time to really look at these lymphatics. 04:37 So there are a lot of areas, and lymphatic chains, and lymph nodes that can drain the breast. 04:45 Posteriorly, we may have drainage to intercostal lymph nodes. 04:50 Mediately, we might have drainage to parasternal or internal mammary lymph nodes. 04:56 Superiorly, we can have drainage to these ones just below the clavicle called the infraclavicular lymph nodes. 05:05 However, the majority of the drainage is really coming from axillary lymph nodes, making them really the most important ones to know when it comes to breast cancer staging. 05:17 And when we talk about lymph nodes, and breast cancer, and spread of cancer, we use our anatomic knowledge to our advantage to see if cancer has spread. 05:27 So for example, let's consider a situation. 05:30 We have a breast tumor here, in this upper outer quadrant. 05:34 We know that there are axillary lymph nodes here. 05:37 They're going to drain into something called the right lymphatic duct that will eventually enter into the venous system via the internal jugular vein where it joins to form the brachiocephalic vein. 05:51 When we say a sentinel lymph node, that's not a fixed thing. 05:54 What a sentinel lymph node is something clinically important to us because it's whatever nodes are going to be the first in this pathway that would drain the area that the tumors in. 06:08 And so that way, those are the areas that are most high risk for spread. 06:14 So, how do we go about finding the sentinel lymph nodes if it depends on the location of the tumor? Well, what we can do is inject a radioactive dye in the area of the tumor. 06:27 And basically let the lymphatics in that area drain to the nearest lymph nodes. 06:34 And then using a little bit of a radioactive probe, we can get generally into the area of those nodes, cut down and look in and see which nodes have taken up that dye. 06:45 That will tell us these are the first nodes in that pathway from the tumor. 06:50 And those nodes can be taken out and sent to a pathologist and can be determined whether or not they do or don't have involvement by tumor spread. 06:59 And that way you can stage the cancer and know that if it hasn't spread there it is not spread to any of the lymph nodes beyond this point.
About the Lecture
The lecture Anatomy of the Breast by Darren Salmi, MD, MS is from the course Thorax Anatomy.
Included Quiz Questions
Which quadrant is nearest to the axillary tail?
- Upper outer quadrant
- Upper inner quadrant
- Lower outer quadrant
- Lower inner quadrant
- Central quadrant
What tissue makes up the majority of the breast volume?
- Fat
- Lobules
- Milk
- Suspensory ligaments
- Muscle
Which artery does not supply blood to the breast?
- Phrenic artery
- Axillary artery
- Internal thoracic artery
- Superior thoracic artery
- Thoracoacromial artery
Author of lecture Anatomy of the Breast

Darren Salmi, MD, MS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
very well explained by Dr Darren Salmi.. thank you for keeping it short and simple
