Playlist
Show Playlist
Hide Playlist
Abdominal Pain: Signs & Symptoms

-
Emergency Medicine Bord Approach to Abdominal Pain.pdf
-
Download Lecture Overview
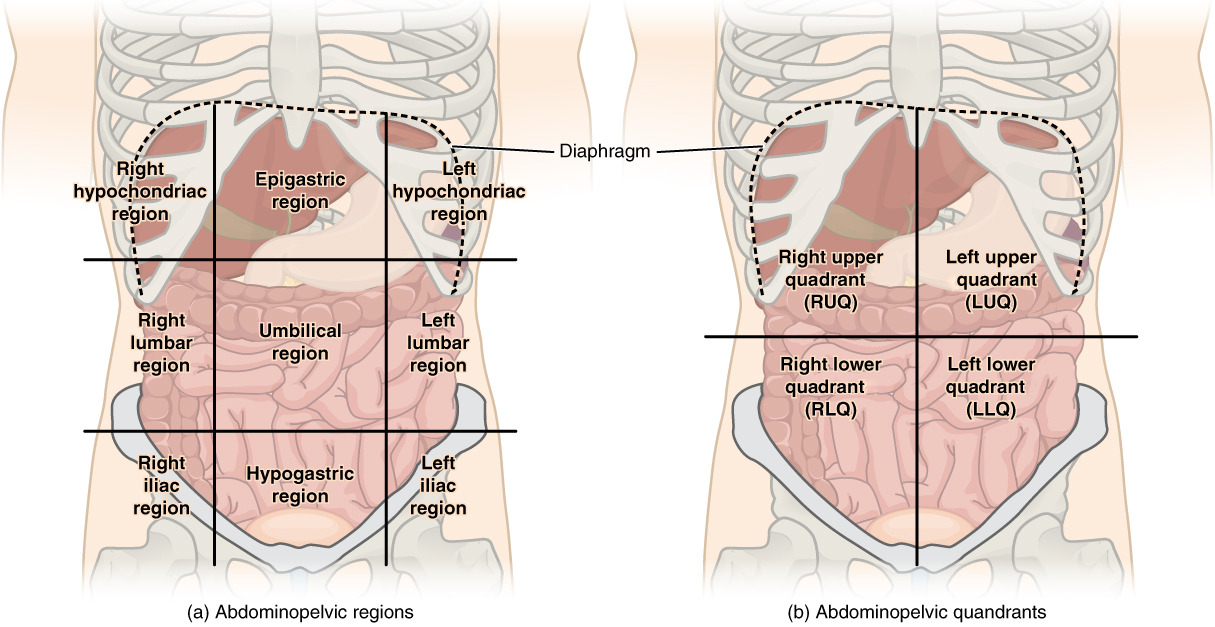
00:01 So abdominal pain is not all created equal. 00:04 There’s different kinds of ways that patients are gonna explain pain and it all has to go back to embryology. 00:09 So it all has to go back with how the organs developed. 00:12 So there is visceral pain and visceral pain originates in the hollow organs and the capsules of the solid organs. 00:19 This corresponds to embryonic development. 00:21 Pain generally related to visceral pain is a dull or achy pain. 00:26 Parietal pain is due to stretching or irritation of the parietal peritoneum, so that’s the lining of the peritoneal cavity. 00:37 This pain is generally sharper so it’s more like a sharp or stabbing kind of a pain. 00:41 Then, the referred pain is the last kind of pain. 00:45 Referred pain is felt at a site far from the diseased organ. 00:49 The classic thing that we think about when we think about referred pain is gallbladder pain felt in the right shoulder. 00:55 So when someone has cholecystitis or potentially biliary colic, that pain may radiate to the right shoulder, so you wanna make sure you’re thinking about that. 01:05 For abdominal pain, this is one of those classic times where you wanna go back to your original history taken class whatever that might be and you wanna go back to really thinking about the different factors that are affecting the pain, does the pain radiate anywhere? So this OPQRST phenomenon. 01:23 So, O stands for onset. 01:24 Was the onset sudden or gradual? Because that can point you in one direction or the other. 01:29 P stands for provocative factors or palliating factors. 01:33 Are there certain things that make the pain worse? Does eating make the pain worse? Especially like in gallbladder disease, we think about eating fatty foods making the pain worse. 01:43 Do certain things make it better? Does it get better when you lay on your side? Does it get better when you eat potentially? There are certain things that actually get better when you eat. 01:52 So, thinking about and asking patients about what makes it better, what makes it worse. 01:57 Q is the quality of the pain. 01:59 So, is it that dull achy pain? Is it a crampy pain? Is it a sharp and stabbing pain? So kind of figuring out and having the patient describe their pain to you can be a useful piece of information for you to have that can help you form your differential diagnosis. 02:16 Radiation, does it radiate to the back? The classic thing that radiates to the back is pancreatitis. 02:23 So it goes from the epigastric abdominal area into the back. 02:26 Does it go to the chest? We discuss the fact that myocardial infarction can potentially be on your differential here. 02:33 S stands for site. 02:35 Where is the pain? Our belly? If you’ve done anatomy, is it divided into different quadrants and there’s different stuff that lives in each of these different quadrants? Now, granted some patients don’t always follow the rules but every so often, but for the most part, knowing the site and knowing where they’re describing their pain is helpful. 02:54 Do they have any other symptoms with the pain; vomiting, anorexia, diarrhea, fever? Vomiting and appendicitis can be very helpful to know, did the pain come first or did the vomiting come first? Is there any blood in the stool? All of this stuff can help you figure out what to do. 03:13 The timing, when did it start? Is it constant or intermittent? Colic-y pain like biliary colic or renal colic by definition is intermittent pain. 03:25 It’s pain that becomes more or less severe. 03:27 Constant pain is pain that just stays there constantly. 03:31 Again, helpful to know the way the patient is describing and reporting their symptoms.
About the Lecture
The lecture Abdominal Pain: Signs & Symptoms by Sharon Bord, MD is from the course Abdominal and Genitourinary Emergencies.
Included Quiz Questions
What is the usual description of visceral pain?
- Dull
- Squeezing
- Sharp
- Throbbing
- Stabbing
What is the most common condition that causes pain that radiates to the back?
- Pancreatitis
- Inferior myocardial infarction
- Gastritis
- GERD
- Cholecystitis
Author of lecture Abdominal Pain: Signs & Symptoms

Sharon Bord, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Very nicely detailled information about abdominal pain semiology and I like her voice.
1 customer review without text
1 user review without text
