Playlist
Show Playlist
Hide Playlist
Increased Intracranial Pressure (ICP), Hydrocephalus & Dandy-Walker Variant (DWV)

-
Slides ICPandHydrocephalus Pediatrics.pdf
-
Download Lecture Overview
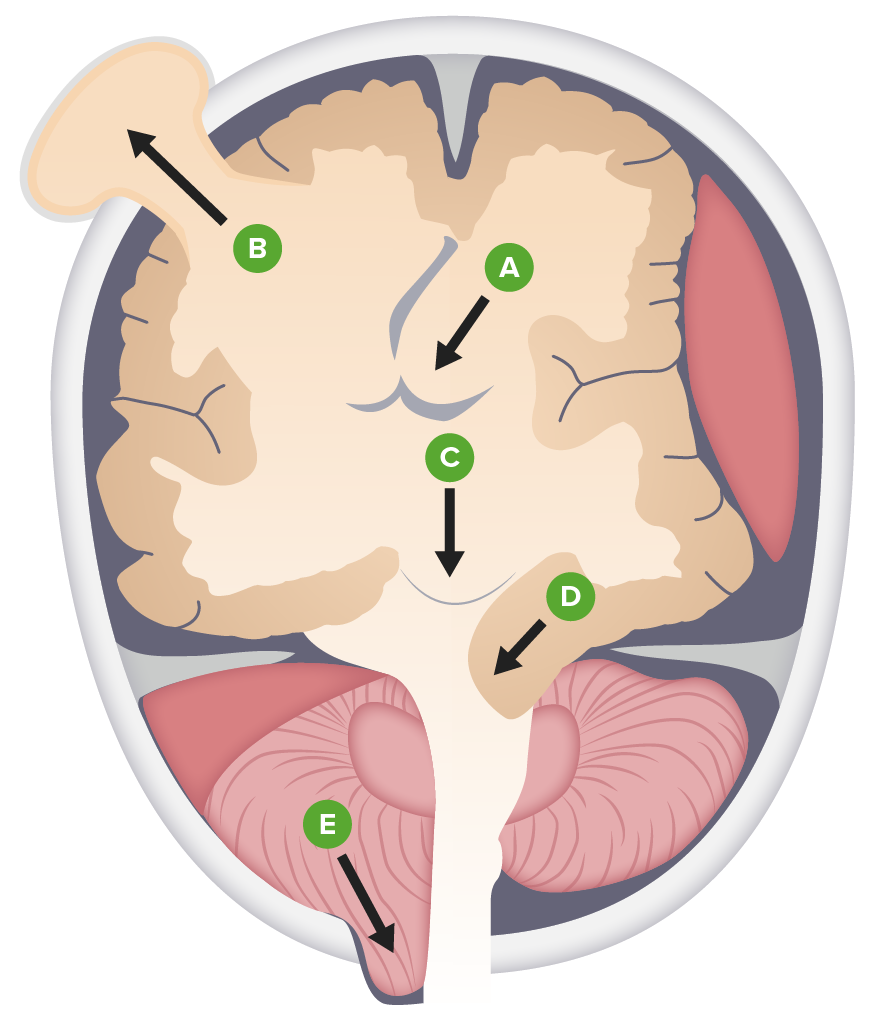
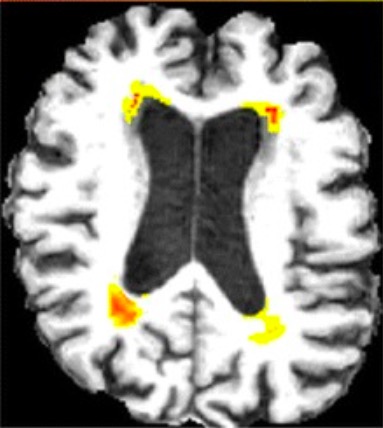
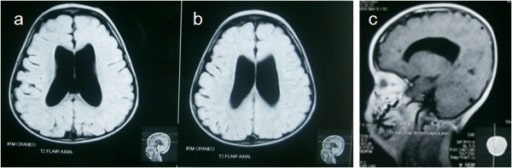
00:01 In this lecture, we'll discuss a variety of problems that happen structurally with children's brain and skulls. 00:08 In particular, we'll focus on hydrocephalus The Arnold-Chiari malformations And Craniosynostosis. 00:16 So, let's start by remembering the basic pathophysiology of increased inter cranial pressure. 00:23 When you see a patient with inter cranial pressure, there are is an expansion of one of the three major components of the brain. 00:30 One maybe brain tissue, another maybe blood within the brain, and another maybe cerebral spinal fluid. 00:37 The normal ICP is about 8-12mm of mercury If this goes up, because of an excessive amount of either brain tissue, blood tissue or cerebral spinal fluid, the problem is that the skull has encased the brain and the only way out for that brain with its increased pressure is down to the foramen magnum. 01:00 The reason why that is a problem is several of the vital areas of the brain such as the pons with regulates breathing and heartrate will be damaged as that brain herniates and it can cause even an instant death. 01:15 So, increased intercranial pressure or increased CSF, is common. 01:23 CSF is made by the lateral ventricles. 01:26 so, those side ventricles are where it is made. It flows down through the ventricles in a system of collecting ducts into the spinal cord. 01:35 It flows down to the spinal column back up and then if flows over the top and it is reabsorbed back to the brain in the dural venous sinuses. 01:47 Adults make and reabsorb a half a litre of spinal fluid a day. 01:52 children a bit less. 01:54 But the point is we are all day long making and reabsorbing this cerebral spinal fluid in large amounts. 02:01 So, you can imagine if there is stricture in the system. 02:04 or a problem with the adequate drainage or reabsorption you can have a problem with increased CSF and that in turn results in increased intercranial pressure And this leads us to hydrocephalus. 02:18 Hydrocephalus has two major varieties. 02:21 Communicating and non-communicating. 02:24 Non-communicating is where the Cerebral Spinal Fluid simply cannot get out of the brain. It is stuck for some reason. 02:32 There are several causes and many of those are congenital and show up in childhood. 02:37 An example would be Aqueduct stenosis. 02:41 Or atresia of the outflow foramina of the 4th ventricle. 02:46 This is called a Dandy Walker cyst. 02:50 Also patients may have a Chiari malformation. 02:53 I'll talk about what these are in a bit. 02:57 Also, patients can develop acquired causes of non communicating hydrocephalus. 03:03 Example would be a posterior fossa neoplasm or a vascular malformation that arises. 03:10 Babies may have communicating CSF in utero. 03:14 But then on their way out suffer an intraventricular hemorrhage. 03:18 that can cause scarring and edema, which can then obstruct the flow of CSF and cause hydrocephalus. 03:27 Also, patients can have a communicating hydrocephalus. 03:30 This is essentially an inability to reabsorb the CSF that's already been produced. 03:38 So, in hydrocephalus, how do patients present? Well, children are more likely to have this than really at any age in the age group. This presents with poor feeding vomiting and seizures. 03:52 But what's key is they will actually have an enlarged head. 03:56 This is one of the major reasons why we screen all children by following their head circumference through the first several years of life. 04:04 This exam will usually show macrocephaly as you can see in this child. 04:11 So, if we are worrying about hydrocephalus, we have an abnormally large head circumference, we then want to scan the child's brain to see what is going on. 04:20 This diagnosis can be made by CT or by MRI. 04:26 CT has the risk of radiation. 04:30 Whereas MRI may have the risk of sedation. 04:34 However, there are new techniques being developed in MRI, where we can assess the vague areas of where the ventricles are enlarged without delving into the details of tissue abnormalities and this can be done relatively quickly. 04:52 Sometimes we can get it done on a baby without sedation at all. 04:56 And that is now becoming our primary modality to both avoid sedation and avoid radiation. 05:04 If a child has a problem with draining CSF out of their brain, regardless of the cause, We are going to help them drain that that brain. 05:14 Because the size of the brain will continue to increase inside the enclosed skull and problems will arise. 05:22 This is where VP shunts come in. 05:25 A ventricular peritoneal shunt is a tube that is implanted into the area of the brain which needs assistance with drainage and then that shunt is tunneled underneath the skin along the back of the skull down along the neck. 05:41 And then it burrows underneath the clavicle and down through the chest into the peritoneal cavity. 05:49 Typically, when they place this, they would put an extra amount of tubing into the peritoneal cavity because as the child grows, this tube is going to be stretched and they need some room for growth. 06:03 After placement, we expect this child to be able to drain the csf and have a cessation of symptoms that is caused by the hydrocephalus such as perhaps vomiting, altered mental status or seizure. 06:17 There is some risk with VP shunt placement. 06:22 The first is infection. 06:24 Children with fever and a recent shunt placement need to be evaluated for a potential of a shunt infection. 06:33 And this is a tricky thing because checking the shunt directly for infection with a needle and sampling some of that cerebral spinal fluid out of that shunt actually bears a risk of introducing infection into that shunt. 06:47 So, we need to very careful about who are we evaluating for shunt infections and who we aren't. 06:54 Almost always shunt infections will happen within six months of the operative procedure that placed or revised that shunt. 07:02 In other words, if a patient hasn't had a shunt problems in years, and now they're presenting with fever, it is much less likely that this is a shunt problem. 07:13 Shunts can and do often fail. 07:17 Failed shunts are a common problem for these patients. 07:21 Basically, proteinaceous material are some reason why the shunt either breaks as the child has grown. 07:29 Or there is trauma or it gets clogged up by proteinaceous material and the CSF stops draining. 07:35 In a patient with a shunt, if they represent the findings of increased ICP, we have to check for shunt failure. 07:45 If the shunt is suspected to have failed, then we will obtain something called the shunt series. 07:51 The shunt series is a series of X-rays including the skull and neck chest and abdomen, where we look at the integrity of the shunt through multiple views to look for cracks, or kinks or disconnections. 08:04 If the shunt series is normal, we can say that there hasn't been a disruption in the line but we can't say whether or not a child in fact has a proteinaceous clog that is preventing the flow of the fluid. 08:18 So, on the back of the child's head as you palpate the shunt, you will notice a small reservoir. 08:25 This is a pump. 08:27 The pump has a valve in it. And there are many different type of shunts. 08:31 And I can't go through all the different types of shunts, and how they are designed and how they are pumped. 08:36 But typically there is either a one pump or a two pump system. 08:40 You can pump this shunt through guidance. I wouldn't try it yourself for the first time and what that would do is it will allow you to test whether cerebral spinal fluid is both flowing proximally, and distantly to that valvular area. 08:56 This is a good quick way to check if the child's CSF is draining through the shunt. 09:03 The problem is that pumping the shunt can itself lead to shunt failure. 09:09 So, we don't want to pump the shunt unless we absolutely have to. 09:13 And even then, some practitioners suggests that we should really leave the shunt pumping to the neurosurgeon so that it is accessed less frequently. 09:22 So, don't pump the shunt unless you're stucked. 09:28 Let's move on to the Dandy-Walker variant. 09:31 The Dandy-Walker variant is an unusual type of obstruction of CSF. 09:37 It results on a cystic dilation of that 4th ventricle as you can see in this patient here. 09:43 Very remarkable dilation of the 4th ventricle. 09:47 It is associated with teratogens, and chromosomal abnormalities such as say down syndrome. 09:55 These patients will present very early with hydrocephalus. 09:59 Usually, within the first three months. 10:02 Again, it is treated with shunt placement but it is different because it is not the lateral ventricles that are affected it's that 4th ventricle.
About the Lecture
The lecture Increased Intracranial Pressure (ICP), Hydrocephalus & Dandy-Walker Variant (DWV) by Brian Alverson, MD is from the course Pediatric Neurology. It contains the following chapters:
- Increased Intracranial Pressure
- Hydrocephalus
- Diagnosis of Hydrocephalus
- Management of Hydrocephalus
- Dandy-Walker Variant
Included Quiz Questions
What is a Dandy-Walker cyst?
- Dilation of the 4th ventricle due to atresia of the outflow foramina
- Dilation of both third ventricles
- A cyst that forms in the cortex of the brain.
- A cyst that forms in the choroid plexus.
- A glial cyst
Which of the following would be a cause of hydrocephalus?
- Aqueductal block.
- Diffuse axonal injury
- Increased arachnoid villi
- Decreased CSF production
- Decreased irrigation of the brain
Which of the following is FALSE regarding increased intracranial pressure?
- Cranial contents can herniate through the foramen spinosum.
- The CSF is produced by the lateral ventricles.
- The normal intracranial pressure is 8-12 mm Hg.
- The CSF is reabsorbed in the dural venous sinuses.
- Adults make 500 ml of CSF a day.
Which of the following is NOT a presenting feature of hydrocephalus in children?
- Mental retardation
- Poor feeding
- Seizures
- Macrocephaly
- Vomiting
Which of the following is FALSE regarding VP shunts?
- The risk of infection after placement is very high during the first 2 years.
- VP shunt can clog up.
- If the shunt fails, a series of x-rays must be taken to assess the integrity of the shunt.
- VP shunt is a connection between the ventricles and the peritoneal cavity.
- Pumping the shunt can lead to shunt failure.
Which is the best management option for a Dandy-Walker cyst?
- Shunt placement
- Mannitol injections
- Needle aspiration of the cyst
- Probenecid
- Fibrosing lateral ventricles
Author of lecture Increased Intracranial Pressure (ICP), Hydrocephalus & Dandy-Walker Variant (DWV)

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Like the details about shunt problems. Amazing lecture. Thanks a lot.
Excellent lecture, this topic is well explained from physiopathology to management. Thanks!
