Playlist
Show Playlist
Hide Playlist
Depth of Burn

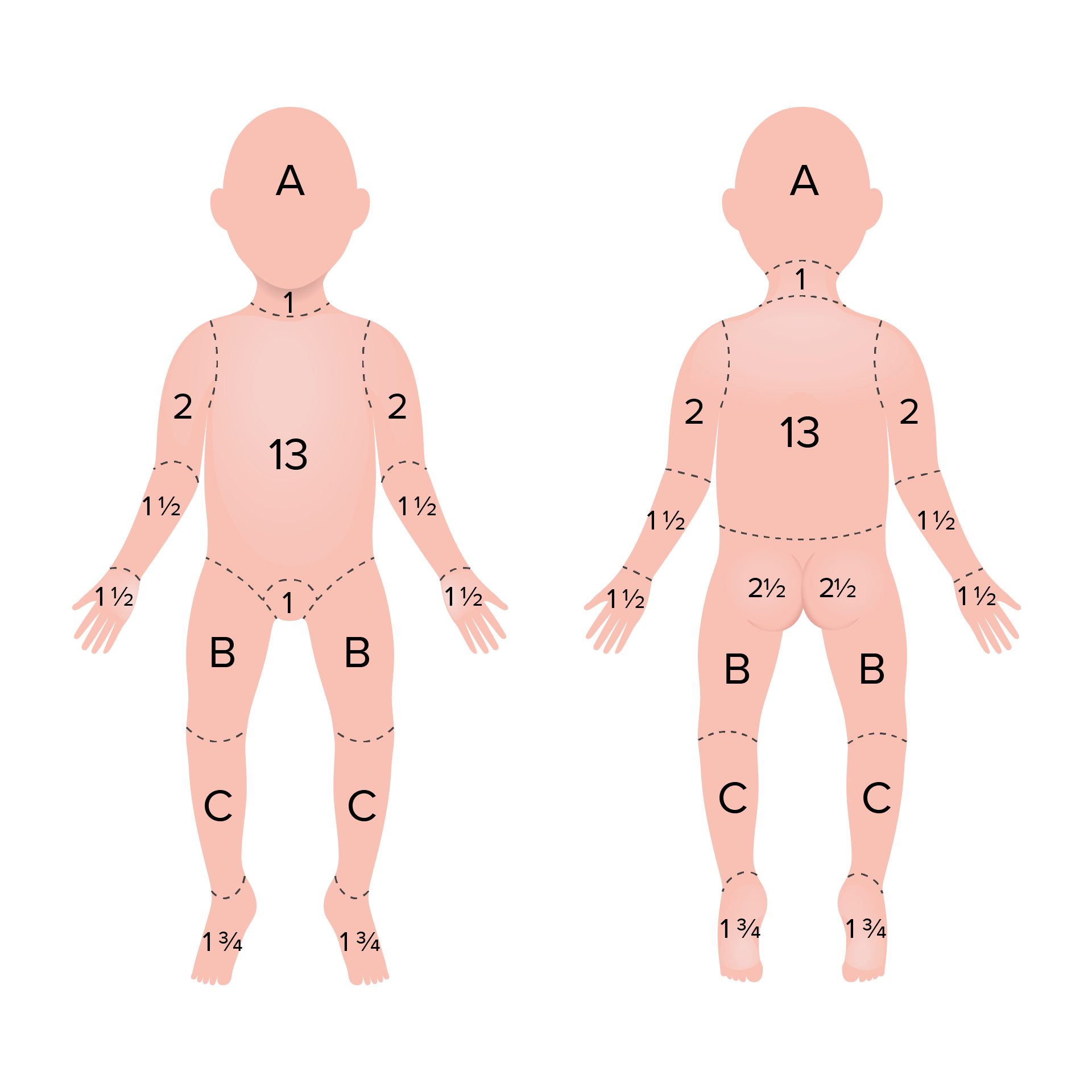
00:00 Okay, this slide will be available for you to view as well. 00:03 This is a good slide because it gives a very good a... 00:09 full chart on what do you expect to see. 00:12 This is what they give in the exam. 00:13 This is taken from the exam question. 00:16 This exactly is what they give and ask what you think it is. 00:20 Okay, so whenever you get anything, no blisters, superficial, blisters, superficial partial thickness, blisters may be present deep partial, but then you are going more towards a full thickness area. 00:34 Definitely, no capillary refill. 00:36 Okay, and that is painless, leathery skin, loss of capillary refill. 00:48 Say it again, Lo. 00:51 Oh, no, no, no, this much as 1%, whole limb is 9 percent, right? Yeah. 00:59 So same with the leg as well, bit of the like 3% 4% 1%. 01:04 Yeah, the whole of the leg is 18%. 01:11 You're intrigued or you're... 01:14 Okay, Fluid Management. 01:17 Probably, you know, that's the most important thing that burn, now the question in your exam will be why is it important? Why is fluid management important is very simple logic. 01:27 You have three zones in a burn. 01:29 You have a zone of coagulation in the middle, surrounding into the zone of stasis and the zone of hyperemia. 01:36 So zone of coagulation is where the maximum heat is conserved. 01:40 That is the maximum, that's the area where it's burned the most. 01:44 Now, if you resuscitated the patient adequately, the zone of stasis is preserved, doesn't expand. 01:52 The patient is inadequately resuscitated, that zone of, zone of coagulation expands. 01:59 So in other words, we have a patient coming in with 18% burnt any. 02:05 You delay for hours by not resuscitating them. 02:08 They'll end up with 35%. 02:11 Okay, that's a whole concept. 02:14 So that's why fluid resuscitation is extremely important not just for their physiological status, but also to make sure the burn does not increase in body surface area. 02:26 Got that? Okay. 02:31 Another physiology question. 02:32 Which comes up either in burn, critical care or in real physiology? You need to know the difference between those. 02:44 Okay. 02:50 So that's a blood vessel. 02:53 So this is intravascular volume, and this is extravascular space. 02:59 Similar to our Monro-Kellie principle, the fluid between the intravascular space and the extravascular space has to be constant. 03:08 How is it maintained constant? By four forces. 03:13 Two inside and two outside. 03:16 So, you have the hydrostatic pressure and the oncotic pressure, hydrostatic pressure and the oncotic pressure. 03:28 Both sides. 03:29 This is capillary. 03:30 This is interstitial, on the tissue. 03:35 Simply put if you are a lot of fluid here, that will go and leak out. 03:41 So how do you prevent that happening? We increase the colloid osmotic pressure by giving more colloid. 03:47 So that fluid will be pulled back in. 03:49 So how is it relevant in burn? It's relevant because when you have a patient with a burn, what do you do? You give them fluid. 03:55 You're not really worried about all these pressures. 03:58 You just need increase the circulating volume. 04:01 So, normally you end up giving nearly three times some more fluid than the patient really request physiologically. 04:10 But at that point you're not worried about that. 04:12 You just need to make sure the circulation is maintained. 04:15 So you end up giving more fluid. 04:16 So you increase the capillary hydrostatic pressure. 04:21 After 6 hours, 8 hours, because burn is a critical assault. 04:26 These endothelial cells will start becoming a leaky. 04:29 So that's called leaky capillaries and the fluid will begin to leak. 04:34 Okay. 04:36 So after 24 hours, you convert your crystalloid to a colloid, by increasing the oncotic pressure. 04:43 So that whatever fluid is lost will be pulled back in. 04:48 So, hydrostatic pressure pushes the fluid out, and the oncotic pressure pulls it back in. 04:55 This is exactly what happens in the RDS in the lung. 04:59 Same concept, anywhere you are giving more fluid. 05:02 If you are asking about fluid challenge CVP monitoring, capillary wedge pressure. 05:07 This is the concept they're looking for, whether you if you understand this, you understand, why you'd give a fluid challenge. 05:13 Why are you why do you give gelofusine. 05:16 Why do you do a crystalloid, okay? Is that clear? I'll give you 30 seconds to make sure they got that right. 05:29 You will seem a bit worried. 05:31 It just middle finger going up, I was thinking. 05:34 No. 05:35 Okay. 05:35 So, this is why you start off with crystalloid, the first 24 hours, and then you move on to colloid. 05:42 Okay, Absolute values, you need to remember for the exam. 05:49 Fluid resuscitation any child, sorry. 05:51 Any child more than 10% body TBSA burned and any adult more than 15% needs fluids. 05:59 That's a standard rule, okay, and that is guided by blood pressure, pulse, temperature, urine unit output, CVP. 06:11 To the body surface area, yeah. 06:14 Okay. 06:17 Parkland's formula we said, always remember this Crystalloid. 06:21 He says 3 to 4 ml. 06:24 When do you give 3? When do you give 4? What is the range? Okay, fair enough, so extremes of each? Comorbidities, I'll take both of those. 06:44 What else? Degree of burn. 06:48 If the majority of areas full thickness you go for 4, If there is an associated inhalation injury you go for 4, and if it is an electrical burn you go for 4. 06:59 The reason being that are occult burns you are not able to see. 07:02 So patient may have say 24% on the skin, but the muscle is burnt or the lung is burnt, or the majority of deep dermal, then you go for 4. 07:14 Otherwise, it's safe to start with 3. 07:18 So 3 indications for 4 ml + extremes of age and significant comorbidities. 07:27 Now this is what I was explaining before, first 24 hours is crystalloid, beyond that you go for colloid, human albumin solution. 07:36 Don't worry about this, they will not ask you. 07:39 But they will ask you, they may expect you to know that. 07:48 Okay, this is why in the UK, the EMSB (Emergency Management of Severe Burn) guidelines, specifically says crystalloid, colloid that's order and that's it. 07:58 No debating in that. 08:00 I agree, there are some units in for example in Swansea. 08:03 They sort of on colloid straight away, but then that's a unit protocol. 08:07 But for the purpose of your exam stick to crystalloid then colloid. 08:12 Inhalation burn, very important for the purpose of your exam. 08:16 History, symptoms, signs, very logical. 08:20 If we have a fire in this room, all of us we get inhalation burn. 08:25 And these are the symptoms, there is nothing really, you know to memorize. 08:30 If you think logically you'll just get a good burn, the face, hair, nasal hair. 08:35 Okay. 08:36 Why is it important? Carboxy hemoglobin has got a 240x affinity for oxygen compared to hemoglobin. 08:45 So because of that, if the patient is breathing room air, it takes nearly 4 hours for them to exhale it. 08:52 But if they give a hundred percent oxygen, the whole thing is exhaled in 40 minutes. 08:56 So that's why you need to give a hundred percent oxygen, normal level in non-smokers will be 0 to 10, 0 to 5 is allowed, more than 10 in smokers truck drivers, etc. 09:11 That's it. 09:23 Okay. 09:26 Escharotomy. 09:29 Circumferential deep burn. 09:31 So to the check. 09:33 Sorry, chest, neck, limb, digit. 09:35 In the forex do a shield pattern, you go through the axillary line axillary planes. 09:42 Then you go on the neck and under the rib. 09:46 Special pattern in the arms and legs, the pre and the post auxiliary lines. 09:53 We discuss escharotomy versus fasciotomy. 09:59 Okay, now. 10:02 Let me get this clarified here because we always see people get confused with in percentages. 10:09 I said fluid resuscitation that is 10% in a child, 15% during in an adult. 10:15 But referral to the burns unit, the threshold is much lower. 10:20 Any 5% in full thickness has to be referred, 5% in a child and 10% in an adult. 10:27 Don't get confused between this and fluid resuscitation, they are different. 10:32 Okay, and all of this. 10:33 You know burns is so specialized in the UK and pretty much everything gets referred. 10:39 So you don't really have to memorize but just remember these numbers. 10:49 Okay. 10:50 Now I'm not going to spend any time on this slide but this has been asked, this is I would classify this as one of the ten percent you can take a chance. 10:59 Nutrition has been asked in burns, but then it's it's quite tricky to memorize, you know. 11:12 Full thickness burn in the leg, no peripheral circulation. 11:17 Yeah, it has to be fully. 11:19 No, not automatically, circumferential full thickness, circumferential and there is no distal blood flow. 11:28 Similar to the fingers. 11:30 You can get a full thickness here, like this tunic effect. 11:33 No, no blood flow. 11:34 So you need to release on the sides. 11:39 For mechanical, for ventilation, trunk and the neck. 11:43 Yeah, it has to be full thickness. 11:46 If this is not full thickness the rest of the unburnt area with sufficient to allow them to breathe for circulation. 11:53 It has to be circumstantial, full thickness. 12:00 No, face, you don't, because you don't have the facial planes like that. 12:04 So we don't do for the face, no. 12:06 Solely for neck, thorax, neck, trunk, limbs. 12:11 Okay, prognosis depends on age, burn size and inhalation injury. 12:15 This is a rough predictor of mortality, okay. 12:18 This... spend about 30 seconds on this. 12:21 Five-year-old child with the 10% burn has got a 15% mortality. 12:26 But a ninety-year-old adult with just a 10% burned, close to 100% mortality. 12:32 Okay. 12:33 Now, this might sound quite extreme which is true. 12:36 For example, you can have a very healthy 90-year-old. 12:39 Who can survive a 20-30% burn. 12:43 It's quite unlikely, usually by the DH, what we always see you get a very fit 70-80-year-old coming with a 12-13% burnt. 12:53 You think well 13% no big deal 80-year-old. 12:56 The moment they have a massive insult like that, the whole physiology crumbles and they just won't recover from that and maybe start with a little bit of pulmonary edema, going on to cardiac failure, going on renal failure, and that's it. 13:10 So the age is very crucial in a burn. 13:15 Okay effects upon a patient pretty much every system is affected. 13:19 Okay. 13:20 Anything else?
About the Lecture
The lecture Depth of Burn by Stuart Enoch, PhD is from the course Trauma and Post-OP Management.
Author of lecture Depth of Burn

Stuart Enoch, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
