Playlist
Show Playlist
Hide Playlist
Obstructive Congenital Heart Lesions – Congenital Heart Disease

-
9 Lecturio Congenital Heart Disease DLM v001.pdf
-
Download Lecture Overview
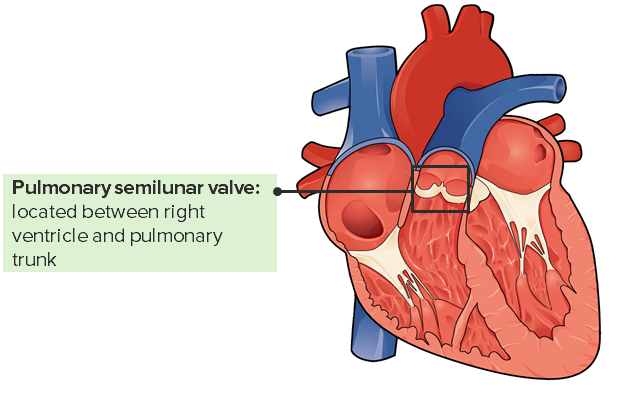
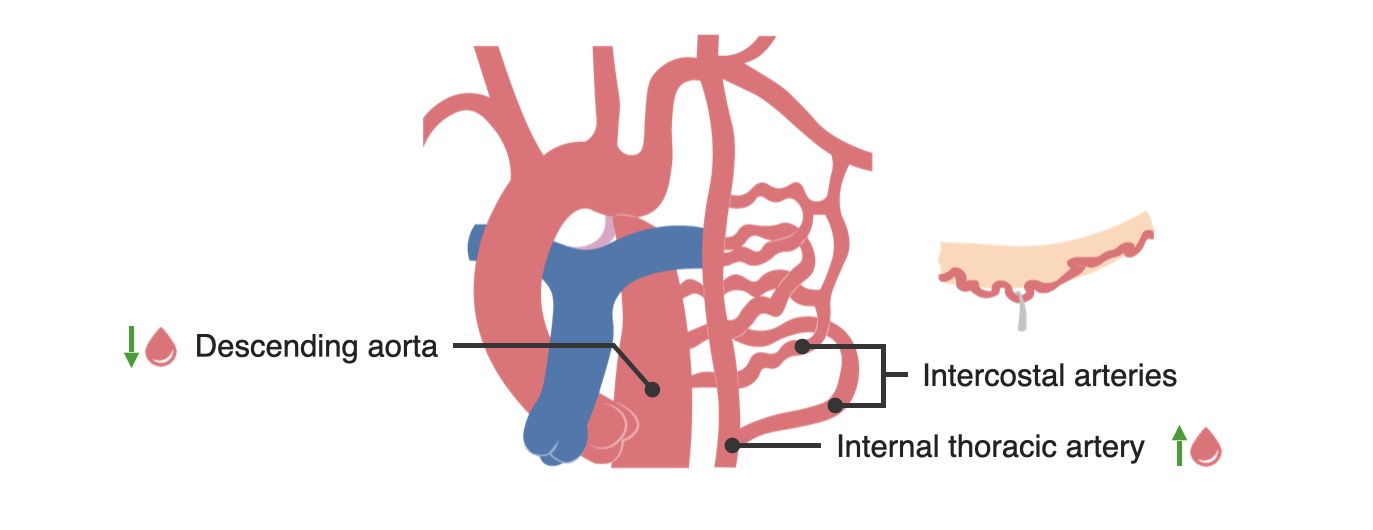
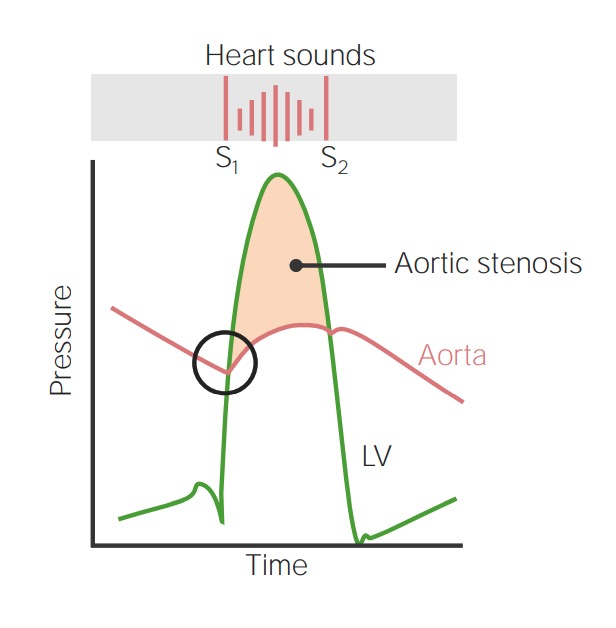
00:00 fatal in early childhood. All right, so let’s start by talking about obstructive lesions. These are lesions that impair the forward blood flow out of one of the ventricles. There are three common ones - pulmonic or pulmonary stenosis in which the pulmonary valve is abnormally formed and consequently, the right ventricle is usually hypertrophied, it has a much bigger workload, and often, the blood flow into the lungs is reduced. If this is very severe, it has to be dealt with in very early childhood, often with a balloon catheter that dilates up the pulmonic valve. Later, the valve may need to be replaced if it scars down a lot. The same thing can happen to the aortic valve. 00:43 It can be born too small and again, this leads to marked decrease in the blood flow into the whole body and again, often requires a balloon catheter opening of the aortic valve in early life and again often down the road, you need to replace that valve as it scars down. Coarctation of the aorta is an obstruction that occurs in the aorta where the aorta is markedly narrowed in one place and again, causes decreased blood flow to the lower extremities and to the abdominal organs and consequently, one has to open that, sometimes with a balloon catheter treatment, sometimes with surgery. We’re going to talk about these in a little more detail. Let’s talk about pulmonary stenosis. As I mentioned before, the right ventricle has to hypertrophy - has to get bigger and thicker because it’s facing a big increase in its afterload, in its work. This is… can lead, of course, eventually, to right ventricular failure. Often the pressure is quite low in the lung and the blood flow is quite low in the lung and you may even see, in early life or later life, you may actually see right ventricular failure with edema, with swelling of the abdomen and the legs. Again, this lesion creates a very nice, loud murmur. So, it’s very frequently picked up in childhood and taken care of. If it’s mild, it’s just followed. If it’s severe, a balloon catheter is put in and expanded and opens the pulmonic valve. It makes a murmur like the one with aortic stenosis. You hear… have turbulence during systole, during the contraction of the right ventricle and you hear, “shoo, shoo, shoo, shoo,” over the pulmonic valve. Aortic stenosis, similarly, is a lesion that affects the left ventricle. Left ventricle also hypertrophies, gets thicker because it has to push harder to get the blood out into the aorta, can also be associated with decreased cardiac output, decreased blood flow and even needs operation or a balloon opening of the valve in very early postnatal life that is soon after the baby is born. If the aortic stenosis is very severe, it has to be opened by a balloon catheter or the infant won’t survive. 03:06 Again, it produces a systolic murmur. Each time the ventricle squeezes, you hear, “zhoot, zhoot, zhoot,” as the turbulent blood flow passes through the stenotic aortic valve. 03:20 Coarctation of the aorta is an interesting one because it’s often missed. The coarctation occurs just after the arch of the aorta and consequently, leads to increased blood pressure just behind it so there’s increased blood pressure in the arteries of the arms and the arteries of the head and there’s decreased blood pressure in the legs. So there’s… and also, of course, a characteristic murmur. So, this may be missed by the doctors because we usually take the blood pressure on the arm. So, the blood pressure might be a little elevated, but often you don’t take the blood pressure in little kids and they can have fairly normal development. I’ve even seen patients get into teenage years or even older when suddenly, the heart began to have trouble keeping up with this increased workload. Patients may have been a little short of breath, they may have been a little fatigued or they may be without symptoms, but it was picked up, as I’m going to show you in a moment, by a characteristic finding on the x-ray. The treatment is either balloon opening of the narrowing or operation in which the stenotic or narrowed segment is removed and a graft is placed in there. This lesion is often associated with a systolic murmur heard best over the spine. Why? Because the aorta runs along the spine as it… after it follows the arch and consequently, you may just hear a nondescript little systolic murmur in the front of the heart whereas when you listen in the back of the heart, over the… over the chest, you may hear a louder murmur. The clue is that you have nice, bounding pulses in the arms and almost no pulse in the legs and you say, “How come I can feel a bounding pulse in the arms, I can’t feel it in the legs?” And then, often, a chest x-ray gives you the answer. This is one of the correctable forms of high blood pressure. Most patients with high blood pressure don’t have correctable forms, but this is one of them. And interestingly enough, even after correction, there’s a tendency for the patient to develop high blood pressure that needs drugs to be taken care of. As I said before, it’s due to a congenital narrowing in the aorta, which sometimes slips past the pediatricians and we see these patients in adult life when they end up with hypertension. Now, here is the finding that often is most embarrassing to the cardiologist. Maybe you’ve seen a patient because they had a little hypertension, and you’ve been asked they’re going to have a hernia repair or some minor surgery and you’ve been asked to clear them. “Yes, their heart’s okay. They’ll withstand the operation.” And then in the preoperative chest x-ray, the radiologist calls up with a great, big laugh and says, “Hey, did you guys know your patient has coarctation of the aorta?” How does the radiologist know that? Because when there’s coarctation of the aorta, there’s large number of collateral or reserve blood vessels that open up. Some of these are underneath each rib and what they do is cause… you can see this little notching, this little cavity on the underside of the rib. That’s a characteristic of the collateral blood vessels. It’s picked up on the chest x-ray and if you hadn’t thought the patient had coarctation, it’s rather embarrassing that the radiologist gets to make the diagnosis. If you thought coarctation might be there and you ordered the chest x-ray, that’s okay. But, there’s a significant number of these folks, usually without severe coarctation who slip through into adult life. If the coarctation is very severe, it’s almost always picked up in the pediatric period of time. 07:06 So, now, we’re going to deal with lesions where there’s a hole in the heart. These
About the Lecture
The lecture Obstructive Congenital Heart Lesions – Congenital Heart Disease by Joseph Alpert, MD is from the course Cardiac Diseases.
Included Quiz Questions
Aortic stenosis directly affects which of the given chambers of the heart?
- Left ventricle
- Right ventricle
- Left atrium
- Atriums
- Right atrium
Right ventricular hypertrophy is most likely to be present in which of the following conditions?
- Pulmonic valve stenosis
- Truncus arteriosus
- Ebstein Anomaly
- Coarctation of aorta
- Aortic stenosis
Systolic ejection click is typically seen in which of the following heart conditions?
- Valvular aortic stenosis
- Tetralogy of Fallot
- Hypoplastic left heart syndrome
- Transposition of great vessels
- Truncus arteriosus
Author of lecture Obstructive Congenital Heart Lesions – Congenital Heart Disease

Joseph Alpert, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Perfect lecture, clear presentation efficient concise knowledge. He has great vocals and phonations .
