Playlist
Show Playlist
Hide Playlist
Head Trauma: Clinical Manifestations and Glasgow Coma Scale

-
Slides Head Trauma.pdf
-
Download Lecture Overview
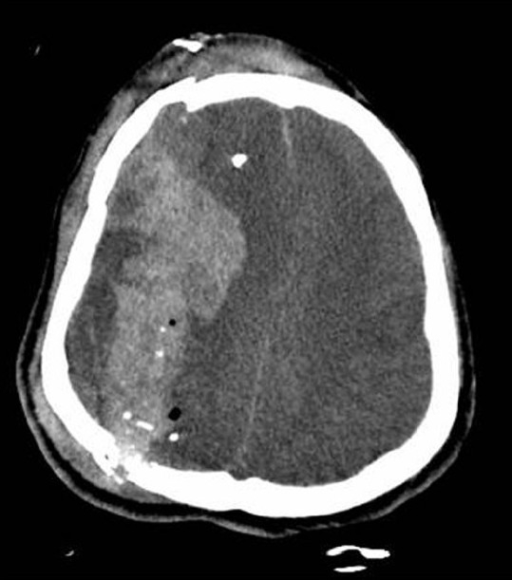
00:01 What about the clinical patient clinical presentation? How to patients typically present from a brain injury? Well our first job is to take a history, a detailed history to explore the type, nature and mechanism of the potential injury and then a comprehensive physical exam. 00:17 In terms of history, we obtained a history of the mechanism of the injury prior to the patient's arrival if possible, bystanders are very important to question in evaluating patients around a trauma. 00:28 We want to look for reported loss of consciousness and for how long the patient may have been consciousness. 00:34 If there was a motor vehicle accident whether the patient was restrained or not restrained by a seatbelt. 00:40 We want to perform a mental status examination and the Glasgow Coma Scale as a standardized and validated measure of the patient's mental status after the time of of a trauma. 00:51 We look for scalp lacerations, palpate for fractures, we're looking to differentiate those open head injuries from a closed head injury. 00:59 And then we want to look for other associated signs that may herald an underlying skull fracture. 01:05 Otorrhea or rhinorrhea, which is CSF fluid drainage from the nose or the ears is highly concerning. 01:12 Clear fluid that is draining from the nose or ears should be evaluated promptly. 01:16 This indicates there's an open connection between the outside world and the cerebrospinal fluid and could be initis for CNS infection and needs to be managed emergently. 01:28 We look for ecchymosis in the raccoon eyes which you can see here which is bruising ecchymosis around both eyes is a specific sign for a base of the skull base fracture. 01:38 And those findings should prompt evidence prompted workup for evaluation of underlying skull fracture. 01:47 We look for conjunctival hemorrhages, blood behind the tympanic membrane or other evidence of underlying trauma. 01:55 And then a comprehensive neurologic exam is key, looking for signs or symptoms that suggest a focal neurologic deficit that requires imaging or other more diffuse deficits that could have occurred from the traumatic injury. 02:11 Next, we want to look at vital signs. 02:13 Vital signs are very important in evaluating a patient with potential trauma and significant alterations in vital signs herald herniation and point towards the concern for herniation. 02:25 Neurogenic shock or hypotension. 02:28 Tachycardia require prompt resuscitation, we really worry if we see vital signs that point towards Cushing's triad, which is hypertension, bradycardia, and irregular respiratory rate. 02:40 And that combination suggests brainstem herniation, or impending modularity brainstem herniation, and is a medical emergency. 02:51 When patients present we use the Glasgow Coma Scale to stratify those patients who are high risk for complications or lower risk. 02:59 The GCS exam addresses the level of consciousness after a head injury. 03:03 Patients receive a score for the best response in each of these three areas. 03:08 Eye opening, best verbal response and best motor response. 03:13 Scores in each area combined, and we get a total score ranging from 3 which is severe reduction in consciousness and function to normal which is 15. 03:23 And you can see each of the three areas, we evaluate the level of eye opening. 03:27 Does the patient open their eyes spontaneously which is a score of 4 or to verbal command or pain or no eye opening? We look at their best verbal responses. 03:37 Is the patient alert, awake, oriented and appropriate in their conversation or are they confused? Are they speaking nonsensically? Are they mumbling or just silence not able to speak? And then in terms of motor response, we want to look at whether the patient is following commands which is normal and a score of 6 or is localizing to pain, withdrawing to pain, has flexor posturing, extensor posturing or flaccid. 04:03 And the lower we get on each score, the more concerned we are about the significance of the injury the patient has received and the more urgent the evaluation is for that patient. 04:13 Let's look a little bit closer at how we stratify these scores on the Glasgow Coma Scale. 04:18 The higher the number, the better the prognosis and this is an important early assessment bedside assessment to stratify short and long term prognosis for these patients. 04:28 A Glasgow Coma score of 9 or less indicates coma. 04:33 These patients need endotracheal intubation for airway protection and aggressive monitoring and resuscitation. 04:41 Glasgow Coma scores in the 11, 12, 13, 14 range indicate minor to moderate injury and a change in score is more important than the absolute scale. 04:50 And so if we see a patient who begins at 11 and is moving up to 12, 13 or 14, that patient is trending in a favorable direction. 04:58 Alternatively, an initial 14 that is declining to 11 requires prompt intervention prior to the development of coma.
About the Lecture
The lecture Head Trauma: Clinical Manifestations and Glasgow Coma Scale by Roy Strowd, MD is from the course Head Trauma.
Included Quiz Questions
What piece of information during history-taking of a patient with head trauma is the most important to ascertain in order to help triage the likely severity of injury?
- Mechanism of injury
- Patient's level of sobriety
- Number of bystanders present
- Patient's baseline functional status
- Patient's ethnicity
What physical exam finding is fairly specific as a clue to a basilar skull fracture?
- Otorrhea
- Scalp laceration
- Nystagmus
- Loss of vestibulo-ocular reflex
- Coma
What are the three signs in Cushing's triad?
- Hypertension, bradycardia, and irregular respiration
- Hypotension, fever, and jaundice
- Scanning gaze, internuclear ophthalmoplegia, and nystagmus
- Confusion, ataxia, and nystagmus
- Urinary incontinence, magnetic gait, and cognitive disturbance
Author of lecture Head Trauma: Clinical Manifestations and Glasgow Coma Scale

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
