Playlist
Show Playlist
Hide Playlist
Biliary Atresia

-
Slides Conjugated Hyperbilirubinemia and Liver Diseases Pediatrics.pdf
-
Download Lecture Overview
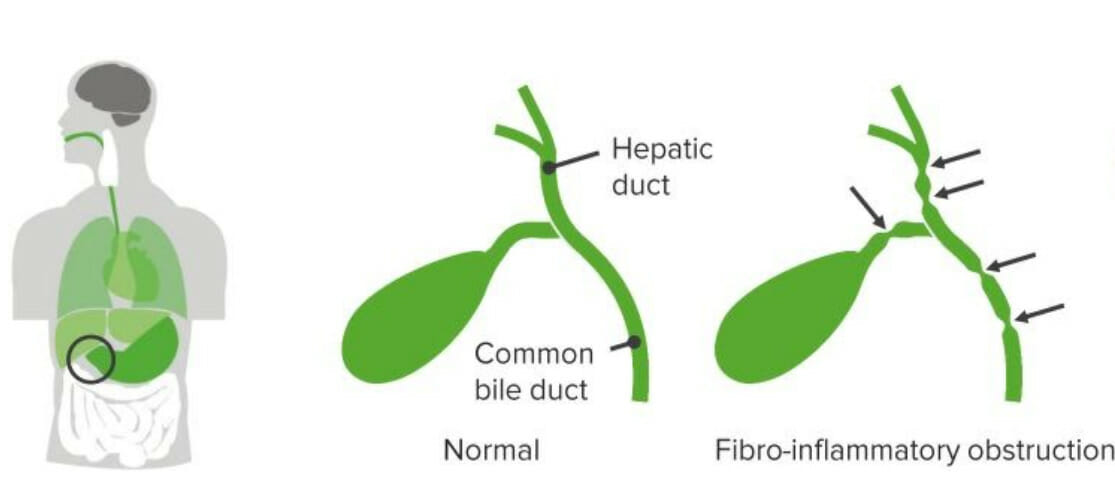
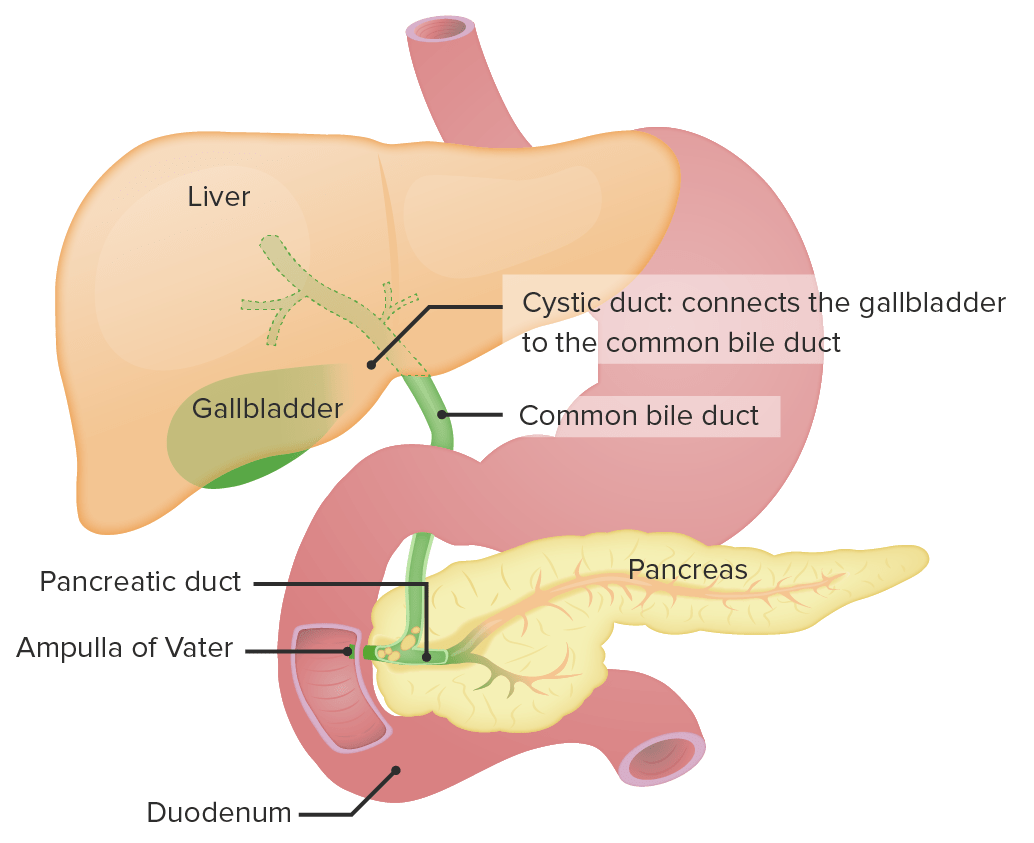
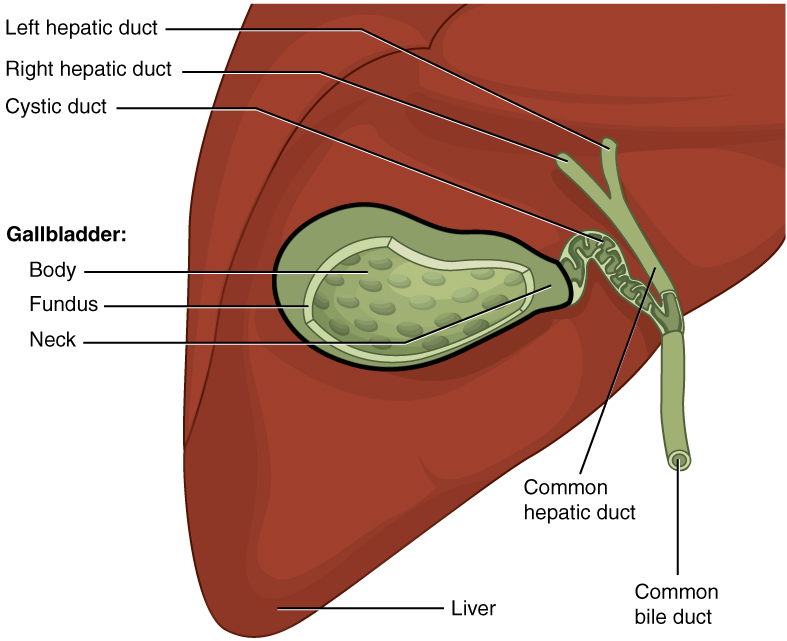
00:02 Let’s move on to another cause of congenital hyperbilirubinemia, which is biliary atresia. 00:09 This is a complete or partial obstruction of the lumen of the extrahepatic biliary tree within the first three months of life. 00:18 A small percentage do present as intrahepatic obstruction. 00:23 So this is not an intrahepatic problem. 00:26 This is an extrahepatic problem. 00:28 And what we typically see as you can see on the left side of your slide is inflammation along the biliary tree with this sort of chain of lakes phenomenon where there are multiple constrictions of the biliary tract. 00:44 So let’s go through how this proceeds. 00:47 Normal development of biliary tree and then patient may have an insult generally perinatally such as a viral infection or some problem that causes the bile ducts to be inflamed, some sort of injury to the mucosa. 01:06 This results in inflammatory response and immunologic response inside the duct and leads to infiltration of the duct and obstruction. 01:16 This duct reaction causes an epithelial proliferation of the cells within the duct which results in a progressive sclerosis and fibrosis of the duct, which thus is going to obliterate these ducts. 01:32 This usually happens within the first month of life and leads to a cholestasis, essentially an inability to get bile through those ducts leading to a backup, which results in hepatocellular injury and a secondary cirrhosis. 01:50 So if you suspect biliary atresia, what should you do? Well, of course, it’s important to take a good history. 01:57 And typically, these are healthy newborns, they’re full term, they have normal weight gain. 02:03 They don’t have a history of a maternal infection in utero because this is an acute thing that happened after birth. 02:11 They’ll have a brief perinatal jaundice and then be jaundice free because that was an unconjugated hyperbilirubinemia. 02:22 And then they develop the jaundice later. 02:25 Generally, it’s a progressive jaundice that happens about eight weeks out. 02:30 And these children will often have acholic or pale stools. 02:34 You’ll see this because the child is not able to extrude the bile, which is the main source of pigment in stool. 02:44 These stools like almost chalky and white in nature. 02:48 The child will also have dark urine because there will be bilirubin levels spilling into their urine. 02:55 On exam, you will of course see the jaundice, you should see scleral icterus. 02:59 But generally, these children are very well-appearing. 03:02 They’re well-appearing children who look okay. 03:05 They’re just turning yellow. 03:08 You may notice a soft hepatomegaly, not a firm mass-like thing, but generally a large liver and they may have a mild spleen as well simply from vascular backup. 03:19 And generally, you get labs and you’ll notice typically their total bilirubin levels around 7 to 10, with a direct level of around 3 to 6. 03:27 And as you can see, this clearly meets criteria for conjugated hyperbilirubinemia. 03:34 They should have a bumped GGT because of that inflammation to the biliary tract and an alk phos, and of course a bumped AST and ALT as well as they’re now developing hepatotoxicity from the bile backup. 03:48 So we diagnose this condition through ultrasound primarily. 03:53 And if there’s more delineation that’s required, we can do a HIDA scan as is pictured above in the first picture. 04:00 Or we can do an intraoperative cholangiogram, which may be useful at determining what type of problem is truly going on. 04:12 The patient is repaired through surgery and a Kasai procedure or a Kasai portoenterostomy is performed where the liver is essentially filleted open and directly anastomosed to a piece of intestine, allowing those multiple ducts to spill directly into the intestinal vault. 04:34 Usually through a roux-en-Y or some sort of similar surgical procedure. 04:40 Transplant may have to occur and that is typically curative of the problem.
About the Lecture
The lecture Biliary Atresia by Brian Alverson, MD is from the course Pediatric Gastroenterology.
Included Quiz Questions
What is the typical finding in a child with biliary atresia?
- Progressive jaundice after 8 weeks of age
- Progressive jaundice from birth
- Severe failure to thrive
- Difficulty with eating at birth
- Kernicterus
Which of the following is the end stage of biliary atresia?
- Cirrhosis
- Chronic hepatitis
- Hepatocellular carcinoma
- Hepatic adenoma
- Sclerosing cholangitis
Author of lecture Biliary Atresia

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Important topic in paediatrics. We had such a case and now I understand better the surgery he's been having. Thank you!
Good coverage of the topic. Hit on important points well. Thank you.
