Playlist
Show Playlist
Hide Playlist
Acute Abdomen: Appendicitis


-
Slides Appendicitis General Surgery.pdf
-
Download Lecture Overview
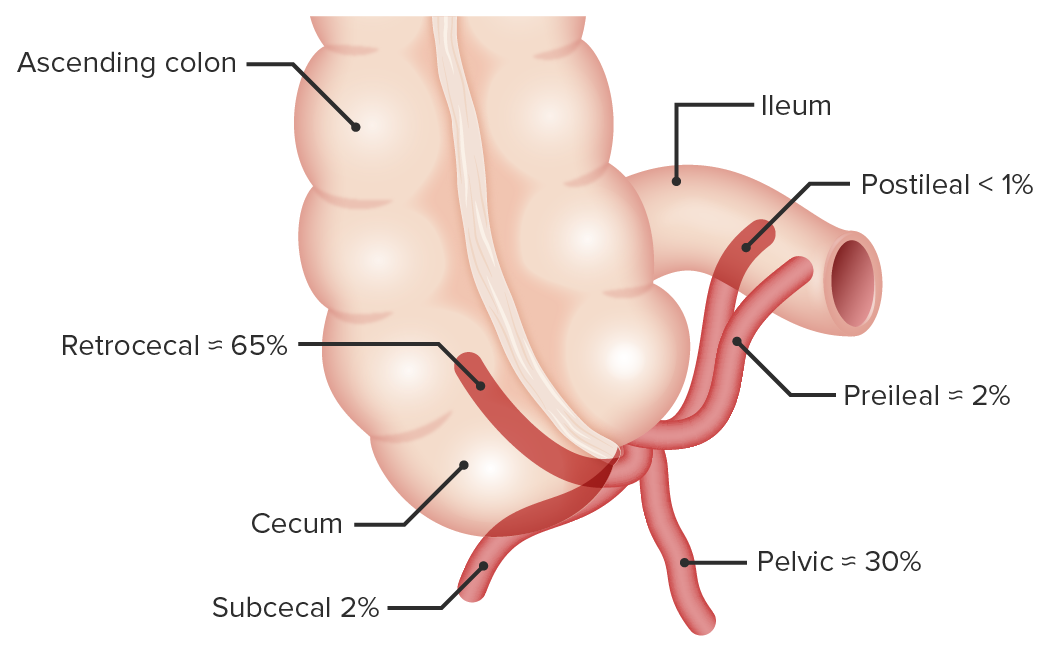
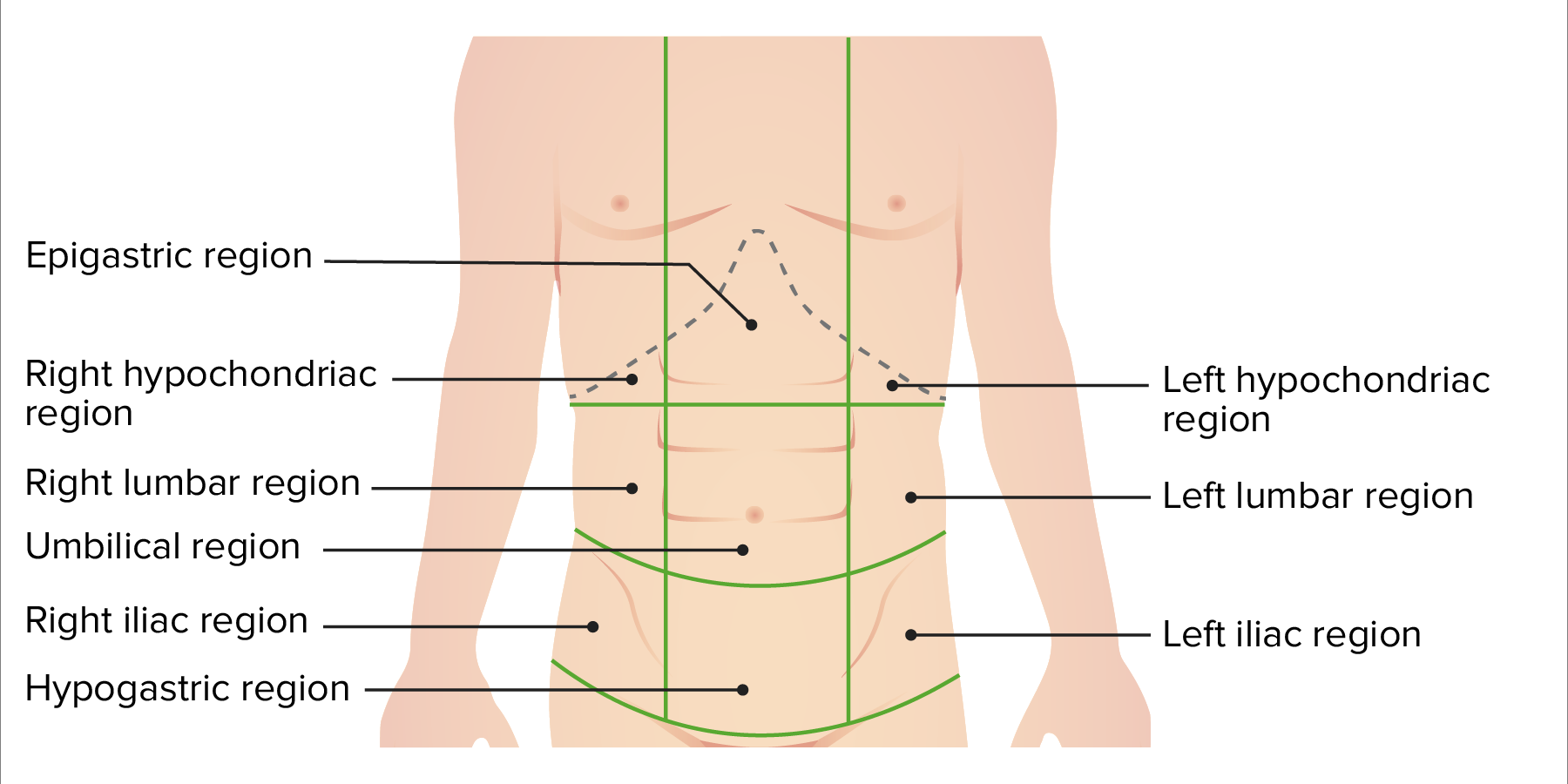
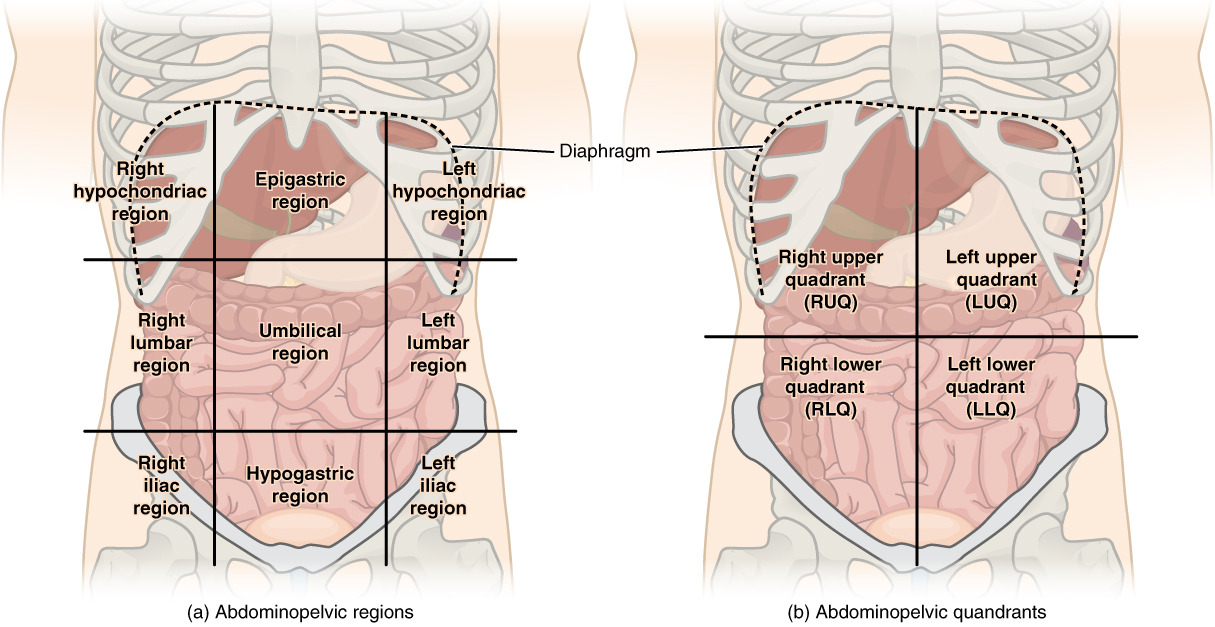
00:01 Hello. Welcome back. Today, we’re going to talk about one of my favorite topics as a surgeon, appendicitis, in the module of the acute abdomen. A patient comes to the emergency department and holds the lower abdomen. I wonder to myself, what’s wrong with this patient. Let’s start with the clinical scenario. An 18-year old man who is otherwise healthy reports worsening abdominal pain that started around the belly button this afternoon. He also reports nausea and has no appetite. 00:37 What’s on your differential diagnosis as you’re seeing this patient in the emergency department? I’ll give you a second to think about it. Of course, you’re thinking appendicitis in this young, healthy man. 00:50 Let’s go over some classic history and physical findings. Abdominal pain, typically described as periumbilical with some radiation eventually to the right lower quadrant of the abdomen. 01:02 Variable nausea and vomiting, again, this is complicated by the fact that when patients present with abdominal pain and nausea and vomiting, we sometimes are thinking small bowel obstruction. 01:14 Very classically associated with anorexia or the lack of appetite, these findings are very classic. 01:21 But remember, as with anything in clinical medicine, not all findings are going to be present. 01:28 Some patients may also report fevers and chills. Let’s discuss the McBurney's point. 01:38 The McBurney's point as you see on this image is defined as a point 2/3 distant from the umbilicus on a straight line towards the anterior superior iliac spine. Peritonitis at the McBurney’s point is what causes the right lower quadrant tenderness classically associated with appendicitis. 02:00 In this image, one notes that one can elicit McBurney's point tenderness even though one is pressing on the left lower quadrant of the abdomen. Recall back to the general principles of acute abdomen that peritoneal irritation sometimes is difficult to localize. Classically, one presses over the right lower quadrant, one elicits the pain at McBurney’s point. This is a classic finding of appendicitis. 02:30 Some other signs you should be aware for the examination, psoas sign. How do I elicit psoas sign to my patient? I ask the patient to lie flat on their bed. I ask them to flex their knee and their hip. 02:43 This is done against resistance from the examiner. 02:46 Another way to evoke the psoas sign is by flexing and extending the patient's right hip while while they lie in the left lateral decubitus position. 02:55 This stretches that psoas muscle. If there’s pain elicited, it's indicative of what’s called a retrocecal appendix. 03:03 Retro, meaning behind; cecal or cecum, the very beginning of the right colon. The retrocecal appendix is not only important for diagnosis of appendicitis but also important in surgical planning. 03:16 It may make the surgery a little bit more challenging. 03:20 Another sign you may want to look for is the obturator sign. 03:24 When the patient lies on his or her back with the leg flexed in the knee and the hip, the physician internally rotates the hip. 03:29 The inflammed appendix, which may be in contact with the obturator internus, causes the muscle to stretch and pain is elicited. 03:35 Lastly the Rovsing sign is reproduced, when pain is elicited in the right lower quadrant during palpation of the left lower quadrant. 03:45 Let’s stop for a second. What special considerations if the patient was a woman that I presented? I’ll give you a moment to think about this. That’s right. 03:57 Gynecologic organs in women can mimic pain particularly in the right lower quadrant that’s very similar to presentation of an appendicitis. 04:05 Let’s go over some of the differential diagnoses of gynecologic organs that can cause similar pain: ovarian torsion, ectopic pregnancy, and pelvic inflammatory disease which is far more common than you think. 04:20 Clearly, the clinical scenario has to fit one of these presentations. 04:24 Pelvic inflammatory disease is particularly important because the management for pelvic inflammatory disease is medicine alone or antibiotics alone versus appendicitis which is something that we would offer surgery. 04:39 So, if you can diagnose ahead of time that it’s pelvic inflammatory disease and not appendicitis, it’s all the better for the patient. 04:45 Ectopic pregnancies are very important to consider. 04:49 This is why in all pregnant eligible aged patients, we get a beta-hCG or urine pregnancy test. 04:57 Most patients get some routine labs. Most of chemistries are going to be not very helpful. 05:04 However, the vast majority of patients who have true acute appendicitis will demonstrate an elevation of their white blood cell count also known as leukocytosis.
About the Lecture
The lecture Acute Abdomen: Appendicitis by Kevin Pei, MD is from the course General Surgery.
Included Quiz Questions
Which one of the following is NOT typically a classic symptom of appendicitis?
- Hematochezia
- Nausea
- Vomiting
- Anorexia
- Fever
Which one of the following is a classic physical exam finding of appendicitis?
- Right lower quadrant tenderness
- Pain only at the anterior superior iliac spine
- Maximal point of tenderness at the umbilicus
- Left lower quadrant pain after flexing the knee and extending the hip
- Cervical motion tenderness
Psoas sign is associated with which position of the appendix?
- Retrocecal
- Pelvic
- Retrocolic
- Subcecal
- Preileal
Author of lecture Acute Abdomen: Appendicitis

Kevin Pei, MD
Customer reviews
3,8 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
1 |
| 3 Stars |
|
1 |
| 2 Stars |
|
1 |
| 1 Star |
|
0 |
Updates filled in the gaps needed for the topic mentioned.
The useful information (the various clinical signs) needed to be better explained or demonstrated.
we need more details for preparing of the USMLE step2 CK.
Every thing is good . Signs and symptoms exactly present in100 persent cases. Very sseful
