Playlist
Show Playlist
Hide Playlist
Abdominal Aortic Aneurysm (AAA): Diagnosis

-
Emergency Medicine Bord AAA.pdf
-
Download Lecture Overview
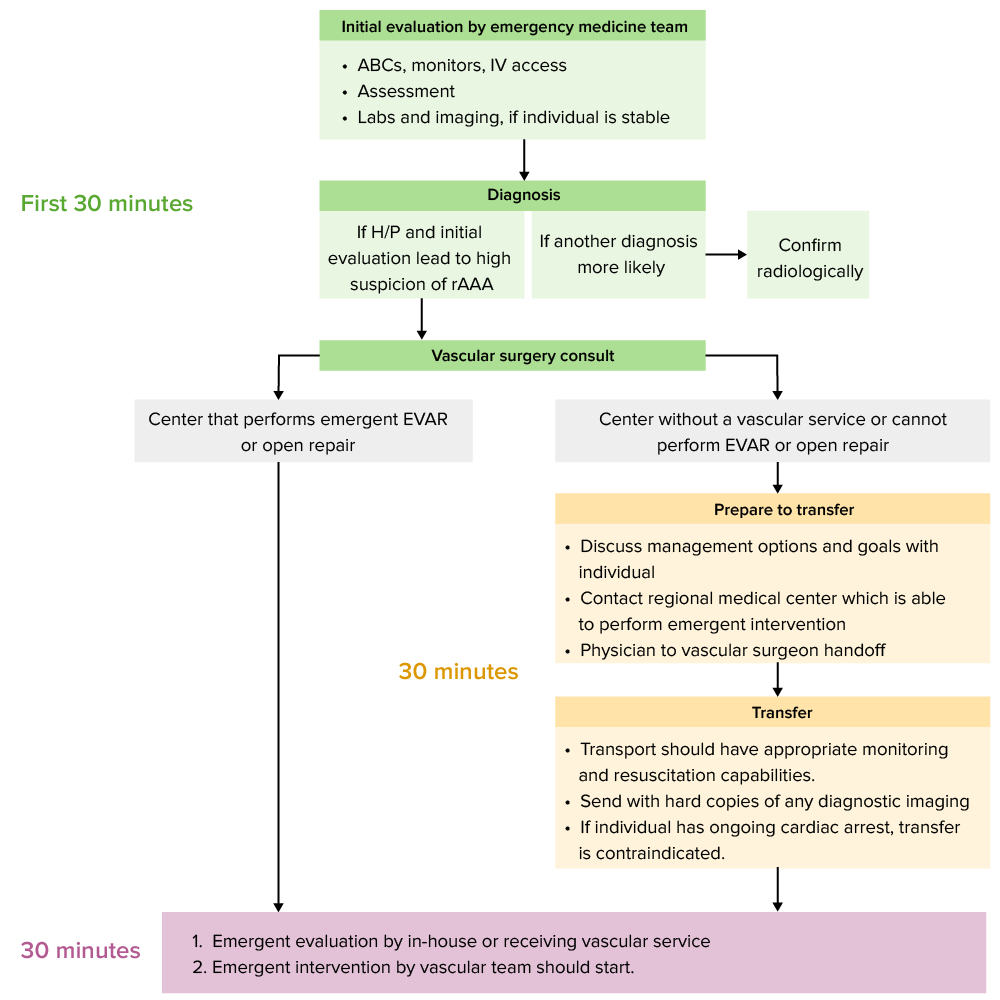
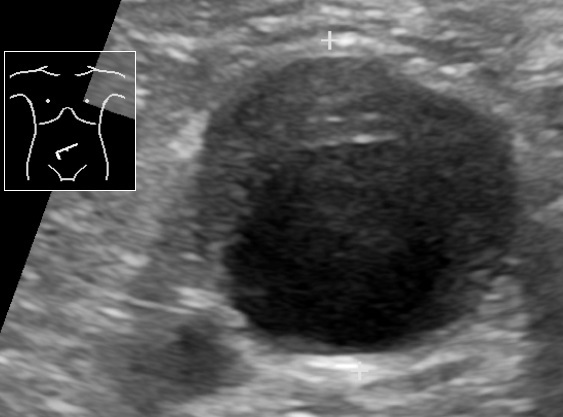
00:01 Now what shall we do for imaging? If you're very worried about this condition or the patient has a known history of AAA and they come in and they’re very unstable. 00:10 One of the first things you wanna do is you wanna get a surgical consultation. 00:14 So you wanna get your surgeon who’s on call on the phone and let them know your concerns. 00:19 You wanna involve them early. 00:21 You wanna make sure that they're aware of your concerns and you wanna make sure that they you know that you potentially want them to come in and evaluate the patient and possibly even take the patient to the operating room. 00:32 The next thing you can do is you can get a plain abdominal film. 00:36 And to be perfectly honest with you this isn’t something that we do super regularly in the ED when we’re looking for AAA, but you can potentially see a calcified aorta. 00:44 And obviously calcification in the aorta will make you concern about further atherosclerosis or disease of the aorta. 00:52 The other testing you can do is CT imaging. 00:56 CT imaging is ideally done with IV contrast. 00:59 And when you do with IV contrast you're able to get the most information. 01:03 Now that’s not to say that if you can't administer IV contrast for your patient that you shouldn't do the test at all because a non-contrast study can actually still give you some information. 01:13 The CT with IV contrast though it’s gonna be the thing that’s gonna give you the best look at your anatomy. 01:20 It’s gonna be the thing that’s gonna show you most accurately whether there's a false lumen, whether the aorta is ruptured. 01:27 It’s gonna give you the most accurate information. 01:31 Ultrasound is the last test or the other test that you should be thinking about. 01:35 Ultrasound is great for patients who have hemodynamic compromise because again, the ultrasound machine can be brought to the bedside of the patient the patient doesn’t have to go anywhere or leave the Emergency Department. 01:46 So if your patient is unstable in any way, this is your test of choice, really. 01:51 It has a greater than 90% sensitivity and it’s technically adequate study. 01:56 Ultrasound, if you remember, is based on whose hands it’s in. 02:00 So it’s based on operator dependence. 02:02 An operator experience. 02:04 So someone who’s very good in performing ultrasounds will likely have a more sensitive test. 02:09 It also depends a little bit on the patient’s body habitus. 02:12 So patients who are obese or overweight or they have a lot of overlying bowel gas from their aorta it may be more challenging to see what you're looking for. 02:20 Just a reminder, the normal size of the aorta in the abdomen is about 3 cm. 02:26 And when we’re looking at the aorta with ultrasound we measure from the outside wall of the aorta to the outside wall. 02:33 You wanna measure on both longitudinal and transverse views. 02:37 So you wanna get a couple of different picture in order to make sure that you know what you're looking at. 02:42 Obesity, tenderness in the belly can definitely limit your ability to perform this because your pushing on the abdomen from the outside. 02:49 And bowel gas may limit the ability to get a good look at the aorta. 02:53 Because of the location of the aorta, all the intestines overlay it. 02:57 So it can sometimes be hard to get that posterior view. 03:01 Again, best for the unstable patient as it can be performed at the bedside. 03:05 And the other thing that’s good about ultrasound is that it’s performed more frequently or very readily by emergency medicine physicians and it’s a big part of our training. 03:13 Sometimes you don’t even have to wait for the ultrasound tech from radiology to come and help you out with that study. 03:19 CT scan again ideally done with IV contrast. 03:24 On the CT scan picture you could see that there is the original aorta which is the bright white area in the center and then the large area surrounding that is the area of aneurysm, that grayish area that surrounds. 03:37 A CT scan without IV contrast still can get you a look but might not necessarily tell you if there’s active bleeding or get you as a good of an anatomy picture as the others. 03:48 CT is a good test for stable patients. 03:51 Because CT while it gives us lots of information and is a great test, the patient still needs to go ahead and leave the Emergency Department. 03:58 One of the worst things in Emergency Medicine physician can ever hear is a code blue or a cardiac arrest patient in the CT scanner. 04:07 That’s something that you never wanna hear. 04:09 You know, it does it happen? It does from time to time, but ideally you wanna make sure that you're selecting those patients who are going to the CT scanner, and that you're sending the appropriate patient to the CT scan because you don’t want your patient who’s unstable to go there and then become more critically ill and have an arrest or a bad outcome in the scanner.
About the Lecture
The lecture Abdominal Aortic Aneurysm (AAA): Diagnosis by Sharon Bord, MD is from the course Abdominal and Genitourinary Emergencies.
Included Quiz Questions
What is the best imaging modality for the evaluation of a possible abdominal aortic aneurysm in a patient with hemodynamic compromise?
- Bedside ultrasound
- Plain abdominal film
- Contrast CT imaging
- Non-contrast CT imaging
- Upright chest film
In the evaluation of a patient with suspected abdominal aneurysm using an ultrasound machine, what is the normal size of the aorta?
- < 3 cm
- 4 cm
- 5 cm
- 6 cm
- 7 cm
Author of lecture Abdominal Aortic Aneurysm (AAA): Diagnosis

Sharon Bord, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
