Playlist
Show Playlist
Hide Playlist
Precocious Puberty in Children

-
Slides Puberty Pediatrics.pdf
-
Download Lecture Overview
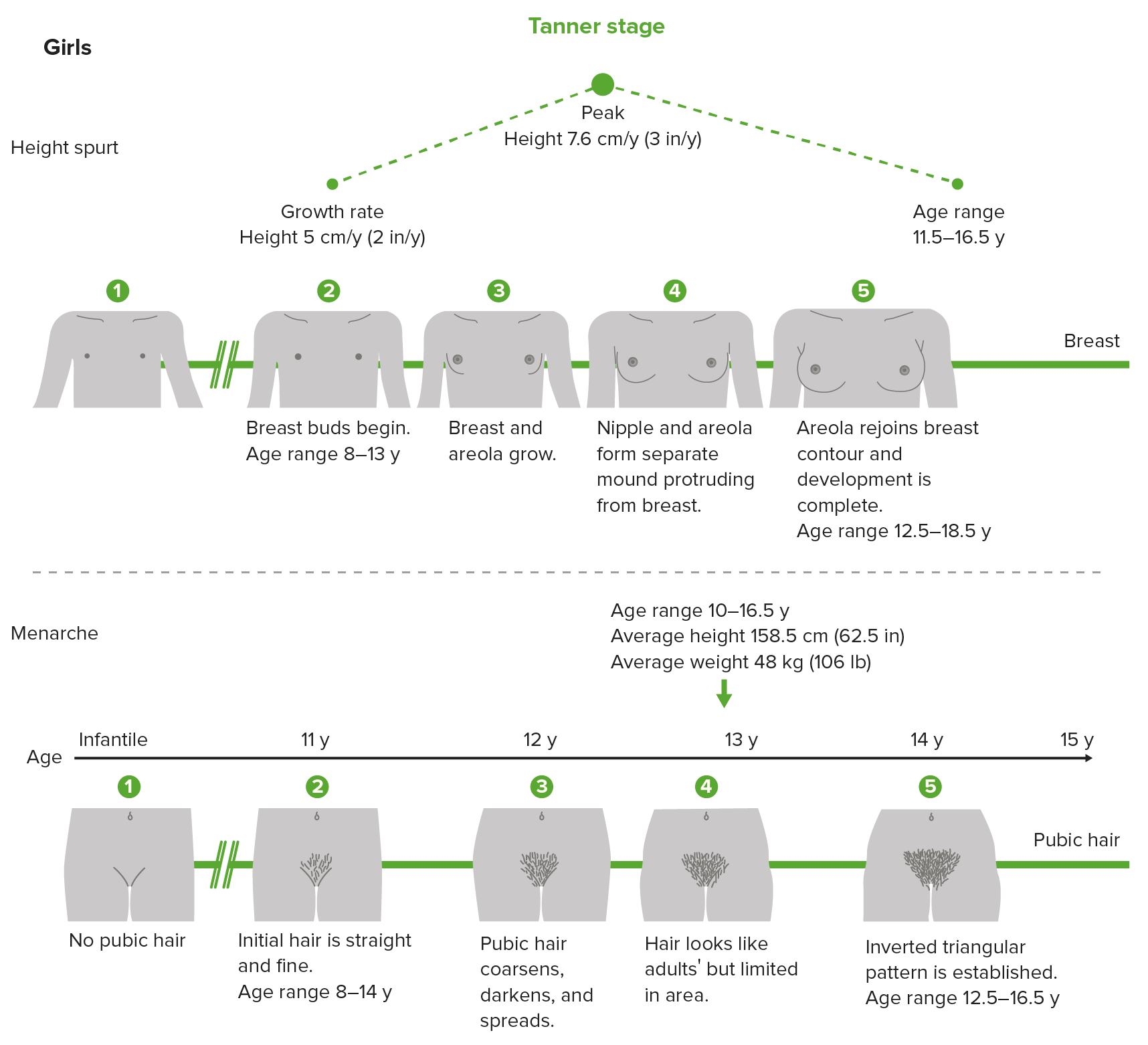
00:01 Let?s talk a little bit about precocious puberty. 00:04 Precocious puberty, unlike benign premature thelarche, is when the full appearance of puberty is happening before the age one would expect. 00:14 Today, children are developing earlier than children used to develop. 00:19 We're not entirely sure why, it may relate to having more hormones in our environment. 00:25 People are taking oral contraceptive pills that gets in the waste water and then is cycled through and we are actually measuring estrogens in drinking water, perhaps that?s the cause. 00:35 It's unclear. But right now, if a boy is developing puberty before the age of 9 or a girl is developing puberty before the age of 8, we consider this precocious puberty. 00:47 So there are two key types of precocious puberty, one is mitigated by a central process and the other is mitigated by a peripheral process. 00:59 Typically in the adrenal glands, or in the testis, or in the ovaries. 01:03 A central process is really in the brain and in particularly in the pituitary gland. 01:08 For central precocious puberty, this requires an activation of the HPA axis or hypothalamic-pituitary-adrenal axis that is resulting in increased levels of LH and FSH. 01:23 This results in elevated testosterone or estradiol production in the genitalia, or the testis and ovaries of the child. 01:32 In girls, 90% of precocious puberty is idiopathic. 01:38 We don?t know why it's happening. 01:41 In boys, 90% of precocious puberty is a result of a CNS tumor. 01:49 An example would be a hamartoma. 01:51 So in boys, we are much more concerned about the possibility of a tumor driving this and in girls this is more likely to be idiopathic. 02:00 Nonetheless, evaluation is likely indicated. 02:05 For peripheral activation, there is no activation of the pituitary gland. 02:11 This is not an activation of the axis. 02:13 This is an exogenous or gonadal excess production of sex steroids. 02:20 There are a lot of reasons why this might be happening. 02:23 Examples are, if a father is using testosterone gel to lift weights and it's rubbing off on a child. 02:30 Other examples might be tumors that can arise such as gonadal tumors in either boys or girls. 02:38 Tumor secreting HCG can cause this. 02:43 Kids with congenital adrenal hyperplasia can develop symptoms where they have excessive sex steroid production because of shunting of hormones across into testosterone. 02:53 There are a number of reasons why this can happen, but key is to understand whether this is peripheral or central. 03:00 So there are some key questions that we can ask to try and break this down. 03:06 First is, we should always ask what was the age of onset of thelarche which is when breasts are developing, pubic hair, growth spurts, and menarche. 03:16 This can create a picture of us understanding. 03:19 We should ask for a history of CNS problems. 03:22 Classic for a pituitary lesion is impingement on the optic chiasm and the subsequent visual problems that you have learned about your neurology courses. 03:31 Any CNS symptom of a mass such as morning headaches, things along those lines, are certainly concerning. 03:38 But it is typical for pituitary tumors to not cause an increase in pressure inside the head. 03:46 So this does not? the absence of these symptoms does not rule out a central process. 03:51 Any exposure to exogenous sex hormones are important to understand. 03:57 Certainly we would like to know if this child is having abdominal pain. 04:01 This may indicate a peripheral tumor such as that?s secreting HCG like a teratoma. 04:08 Any rapidly advancing puberty is indicative of the possibility of adrenal tumor. 04:16 This tend to cause very rapidly advancing puberty and that can be concerning and we might want to just empirically image the adrenal glands. 04:25 So if we suspect precocious puberty and we want to delve into what exactly is causing it. 04:33 The best way to check is to get an LH, an FSH, and in boys a testosterone level, and in girls an estradiol level. 04:41 Typically, in both central and peripheral puberty you will have elevated testosterone boys and estradiol on girls. 04:51 But as would make sense, if it's a central lesion the LH and FSH would be high in central precocious puberty and they would be low in peripheral precocious puberty as there is a negative feedback loop. 05:03 Often in precocious puberty, there is bone delay. 05:08 And if you wanna learn more about how we check bone age delay, you can look at our talk on short stature. 05:15 But generally, we will expect that they are more than 2 years older than their hand x-ray. 05:21 Ultrasound should be obtained to show precocious enlargement of the uterus or ovaries in girls. 05:27 And if suspected, studies should be done to find the tumor. 05:32 So if a child has a high HCG level, we should then go looking for where that tumor is so it might be excised. 05:39 In patients with central precocious puberty, it's critically important to obtain a brain MRI and especially with a cutdown on the pituitary. 05:48 A cutdown is just extra focused high resolution images of the pituitary so we know what exactly is going on. 05:56 Remember that serum HCG is high also in hepatoblastoma, so in those cases evaluation of the liver is indicated from a radiographic standpoint. 06:07 And certainly we're gonna check labs such as 17-hydroxyprogesterone if we suspect the patient has congenital adrenal hyperplasia. 06:16 If you want to know more about that, you can check out the lecture on congenital adrenal hyperplasia.
About the Lecture
The lecture Precocious Puberty in Children by Brian Alverson, MD is from the course Pediatric Endocrinology.
Included Quiz Questions
What is the most common cause of precocious puberty in a boy?
- A CNS tumor
- Peripheral precocious puberty
- Benign premature thelarche
- Exogenous steroid
- Adrenal hypertrophy
What is the most common cause of precocious puberty in a girl?
- Idiopathic
- A CNS tumor
- Benign premature thelarche
- Exogenous steroid
- Adrenal hypertrophy
Author of lecture Precocious Puberty in Children

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent lecture. Endocrinology is often an obscure or not-well explained topic. This is not the case here. Thank you
Nice lecture, but the treatment in boy or girl clinical case...
