Playlist
Show Playlist
Hide Playlist
Duchenne vs. Becker Muscular Dystrophy

-
IRheumatology II 01 Muscle Pathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
00:02
A major type of muscular
dystrophy is called DMD,
or Duchenne Muscular Dystrophy.
00:08
It affects approximately 1
in 3,500 male births.
00:14
Progressive weakness will begin
early as we shall see,
and by the time this young male
reaches the age of 10 or 12, is
already wheelchair bound.
00:24
Why is that?
Well this then goes back to you
understanding the major protein
that I just showed you—the anchor,
one of the largest proteins that
is coated for in our body,
so when it’s so large,
it's actually susceptible to
mutations taking place.
00:38
Now if, if, there is a mutation
that is so severe
in which that protein is truncated
because of a frame shift,
that dystrophin is completely deficient
or not present at all in
terms of functioning,
then you’ve lost the anchor.
00:55
Now if you remember that picture
that I showed you,
where that dystrophin
was a proper anchor between
your alpha and your beta
dystroglycans with your
actin intercellularly,
and you no longer have that,
how in the world are you supposed
to have contraction
in the skeletal muscle and the cardiac?
You don’t. So keep those two in mind again,
and hence, it was important for me
to quickly walk you through
a little bit of anatomy and
a little bit of physio.
01:22
Most common and most severe of
the muscular dystrophies,
it is complete deficiency
of that functioning dystrophin
and it’s on chromosome X.
01:33
The majority of your patients will have
an X-linked recessive issue,
hence males will be affected
obviously much more so
whereas females could then
going to have a trait.
01:43
One third of your patients may
have de novo mutation,
and that mutation you must know,
is a frame shift.
01:50
Why must you know that?
Well apart from the knowing that
it’s important for Duchenne,
what we’re going to do is, is
we’re going to compare
our Duchenne with Becker. In fact,
when we go through our
muscle pathology here
in this discussion,
we will be making a lot of comparisons
between diseases,
we’re making comparisons between
Duchenne and Becker,
and we’ll be making comparisons between,
let’s say, myasthenia gravis and Lambert-
Eaton Myasthenic gravis syndrome.
02:17
So in Becker, it is non-frame
shift type of mutation.
02:22
In Duchenne, it could be
frame shift mutation.
02:27
One-third of your patients, it’s still a
decent percentage of your patients,
both however, Becker and Duchenne,
could have and would have deletions.
02:39
There’s absolutely no dystrophin,
and as you would expect, elevated
levels of creatinine kinase.
02:47
So what about the ladies?
Well, if it’s X-link recessive then it
could be a carrier, a trait.
02:54
There might be high levels
of creatinine kinase
and ultimately the organ to be
susceptible to damage
would be the heart in your young lady,
cardiomyopathy,
and as do patients who survive long enough.
03:08
And that is the thing,
that in a female carrier of Duchenne,
X-link recessive,
that ultimately it’s the heart
that will then weaken to the point of
dilated cardiomyopathy and fatality.
03:22
In Duchenne Muscular Dystrophy, this child,
a boy, born frame-shift mutation
perhaps, X-link recessive,
clinically manifests by the age of
2 to 3 years of age,
has lost ability in the pelvic girdle
to get himself up.
03:41
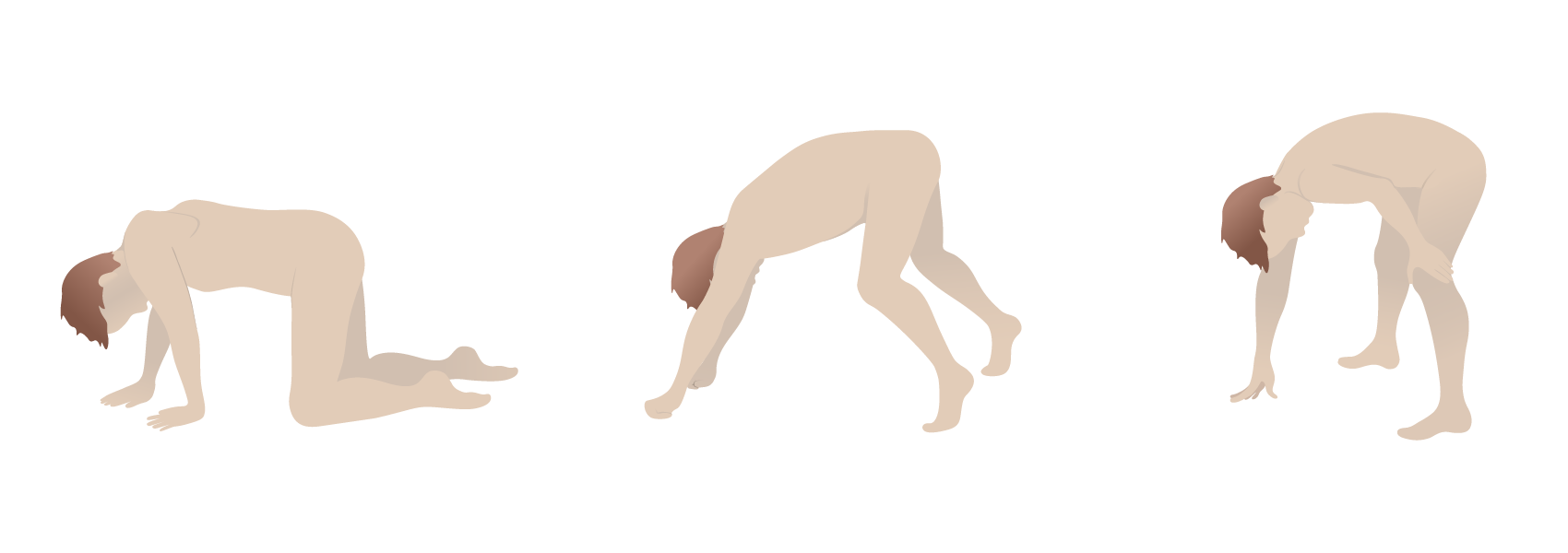
This is the manner in which he does if
you take a look at the picture here—
crawl, and not only crawl,
but because the patient now
is not able to get up,
has to then climb up on himself.
03:53
This is then called, as we shall
see, Gower’s sign.
03:57
In the meantime, down in the calf,
it looks as though that there is
hypertrophy but it's pseudo.
04:02
Remember, there is no dystrophin,
how in the world are you supposed to have
hypertrophy of the skeletal muscle?
It’s not happening.
04:10
So, therefore, what is giving this child’s
calves this hypertrophic appearance?
Pseudofat.
04:20
Right? In other words, you have
fibro fatty changes taking place
so you can imagine now, as I shall show you,
what your skeletal muscle fascicle
should look like
versus what color is fat when you do,
let’s say, a stain on histology.
04:36
Fat—it’s clear, vacuolating, correct?
So could you imagine where you have
muscle fiber that is then
occupied by fat instead—
fibro fatty change—we call this
pseudohypertrophy.
04:50
Now, the issue is there’s so much
weakness taking place
that maybe the diaphragm
can’t function properly,
so therefore, pneumonia is a possibility,
and it’s so bad in the teens
if it was to occur in DMD
that the child may even then
die secondarily.
05:08
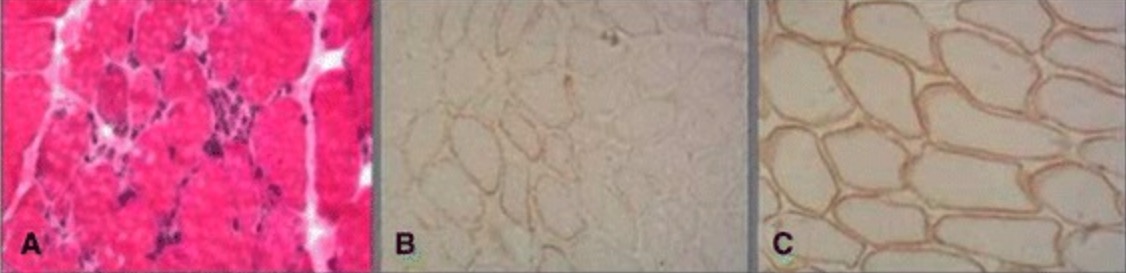
Now characterized by, I’ll show
you histology coming up,
in which the fascicles of your
skeletal muscle
are going to be in different
sizes and shapes,
and some are trying to desperately
regenerate,
successful? Most likely not.
05:25
Gower’s sign is what I’m demonstrating
here for you
or should I say the picture is
demonstrating for you,
in which the child is trying to get himself
up by climbing on himself.
05:39
Here once again is the picture
that I showed you earlier,
and now with better understanding
of what the disease is,
with the better understanding in Duchenne,
as to how that dystrophin anchor
protein that you see there,
you have issues with your alpha
and beta dystroglycans
and if you don’t have a proper bridge
that’s taking place between the
dystrophin and the actin,
then that skeletal muscle or cardiac
muscle is then prone to damage.
06:07
Dystrophin with the largest proteins.
Remind me again,
what kind of mutation could be taking
place de novo one-third of the time?
Frame shift or non-frame shift?
Frame shift resulting in truncated protein.
06:20
Whereas in Becker, as we shall see,
there could be non-frame shift,
it can be non-truncated,
it could have deletions in both,
and X-linked in both.
06:32
I told you that I’d show you a picture,
a histologic picture where you have
different sizes and shapes of the muscle
and exactly what you see here
upon cut section.
06:41
In addition, you also find endomyosin
connective tissue and the regeneration is
what is being depicted here in the middle,
desperate regeneration.
06:50
And it’s the blue hue that you will observe
in this histologic picture.
06:57
Difficult to regenerate.
07:02
Our next muscular dystrophy is Becker.
07:05
Now the most common of the muscular
dystrophy is Duchenne,
and is the most severe,
Becker however,
is muscular dystrophy but it is
less severe than Duchenne
and the reason for that is because
there is partial dystrophin functioning.
07:22
So they’re similar. Deletion is found in both.
07:26
What will you not find in Becker
in terms of mutation?
You will not find frame shift. It’s
a non-frame shift mutation.
07:34
Non-truncated protein.
07:37
The function dystrophin will be
produced in a little bit.
07:41
I’m going to show you
where the representation of dystrophin
can be seen in labs.
07:49
The age onset a little bit later
whereas as I told you about in DMD,
the presentation may start
in as little as 2 to 3,
here maybe about 8 to 25
and unable to walk definitely
by the age of 25,
is the most common presentation in Becker.
08:07
So everything is a little bit delayed.
08:10
The reason for that is because
it’s not that you have
no function of dystrophin, you have
some functioning dystrophin.
08:20
Here’s an important picture,
the first picture here on the left,
I need you to understand, its imperative
muscular dystrophies.
08:30
The 2 muscular dystrophies
to be compared here
will be Becker and will be Duchenne.
08:36
Remind me again, in Duchenne,
are you producing any dystrophin?
No. Frame shift mutation?
So what you’re seeing here,
if you take a look at the normal above,
is normal uniformed muscle fascicles.
08:54
Uniform—not varying in sizes and shapes.
08:58
If you take a look at the
middle row on the left,
you’ll notice DMD stands for Duchenne,
you’ll notice that the outline here,
take a look a little bit closer please,
different sizes and shapes of
your skeletal fascicles.
09:14
Which you notice the very bottom here,
compare your DMD Duchenne,
with BMD which is Becker,
you’ll notice that the Becker
looks better than the DMD as in Duchenne,
you’ll notice some of the muscle
fascicles are not even present.
09:30
The picture there is not as uniformed
as what it is normally up above;
however, with Becker,
it’s trying to look like the normal
control on top
but you can’t in Becker because you have
a deficiency but you still have some
functioning dystrophin.
09:51
Is that understood? That’s the
picture on the left.
09:54
Now the picture on the right
will do the same thing.
09:58
This time, we’ll take a look at the
movement of your dystrophin.
10:04
It’s the movement of dystrophin
from one end to the other
and dark bars that you see here
then represent the supply of dystrophin
in the particular patient.
10:22
We have 3 patients here.
10:24
So on the far right, you’re going to
be focusing on the bar.
10:27
Those bars then represent the
amount of dystrophin
that is present in your patient.
10:33
The controlled patient, you’ll notice
has a dark black bar.
10:39
That represents normal dystrophin—
do not worry about the number 427—
understand that that then
represents dystrophin.
10:46
Remind me in Duchenne, do
you have any dystrophin?
You will not. Do you find any black
bars in that column for DMD?
Not at all.
10:57
And remind me again, when does
the onset of disease begin?
Maybe about 2 to 3 years clinically,
pelvic girdle and such, Gower’s and so forth.
11:07
In Becker, take a look.
11:10
In Becker there is some
functioning dystrophin
and there’s some abnormal dystrophin.
11:17
This tries to look normal but can’t
and here you have issues
with non-frame shift
and deletion taking place,
it is X-linked, it could be X-linked as well.
11:28
That is how you read these 2 pictures
and compare your 2 major
muscular dystrophies.
About the Lecture
The lecture Duchenne vs. Becker Muscular Dystrophy by Carlo Raj, MD is from the course Muscle and Soft Tissue: Pathology. It contains the following chapters:
- Introduction to Duchenne Muscular Dystrophy
- Introduction to Becker Muscular Dystrophy
- Lambert-Eaton Myasthenic Syndrome
Included Quiz Questions
A 3-year-old boy is having difficulty running, jumping, and walking up steps. Physical examination reveals pseudohypertrophy of the calf and a waddling gait. Serum creatine kinase (CK) concentrations are markedly elevated. What is the most likely diagnosis?
- Duchenne muscular dystrophy
- Becker muscular dystrophy
- Polymyositis
- Dermatomyositis
- Poliomyelitis
Which of the following statements about the pathogenesis of Duchenne muscular dystrophy (DMD) and Becker muscular dystrophy (BMD) is TRUE?
- DMD is caused by a frameshift mutation, while the milder BMD is caused by a missense mutation.
- DMD is caused by a missense mutation, while the milder BMD is caused by a frameshift mutation.
- DMD is caused by a missense mutation, while the more severe BMD is caused by a frameshift mutation.
- DMD is caused by a frameshift mutation, while the more severe BMD is caused by a missense mutation.
- Both DMD and BMD are caused by frameshift mutations
Gower sign, seen in a 3-year-old boy who uses his hands and arms to "walk" up his own body from a squatting position due to lack of hip and thigh muscle strength, is suggestive of what condition?
- Duchenne muscular dystrophy
- Becker muscular dystrophy
- Poliomyelitis
- Polymyositis
- Myasthenia gravis
A 16-year-old boy with increasing difficulty running, jumping, and walking up steps over the past several months states he was told his grandfather had similar symptoms when he was young. Serum creatine kinase (CK) concentrations are markedly elevated. Which of the following is the most likely diagnosis?
- Becker muscular dystrophy
- Duchenne muscular dystrophy
- Churg-Strauss syndrome
- Poliomyelitis
- Dermatomyositis
Which of the following statements regarding Becker muscular dystrophy (BMD) is TRUE?
- A patient with BMD has more dystrophin than a child with Duchenne muscular dystrophy, but less dystrophin than an unaffected individual.
- Becker muscular dystrophy has an earlier onset than Duchenne muscular dystrophy.
- Becker muscular dystrophy is more severe than Duchenne muscular dystrophy.
- There is a higher level of dystrophin in a child with Duchenne muscular dystrophy than one with BMD.
- Dystrophin is absent in Becker muscular dystrophy.
What organ is susceptible to damage in a symptomatic female carrier of Duchenne muscular dystrophy with an elevated creatine kinase level?
- Heart
- Kidneys
- Spleen
- Brain
- Liver
Author of lecture Duchenne vs. Becker Muscular Dystrophy

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
