Playlist
Show Playlist
Hide Playlist
Hypercalcemia: Definition & Clinical Manifestation


-
Slides Hypercalcemia.pdf
-
Download Lecture Overview
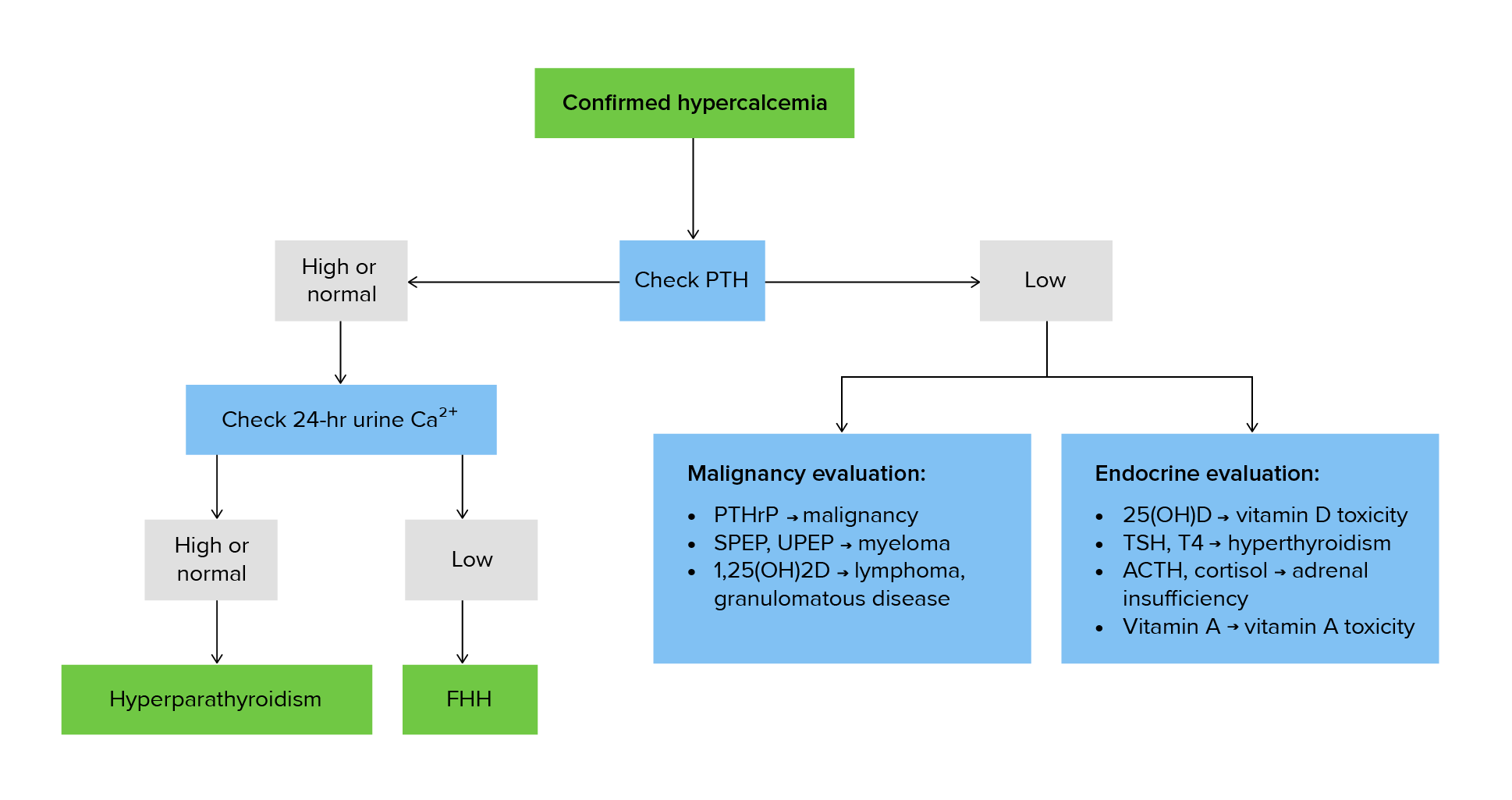
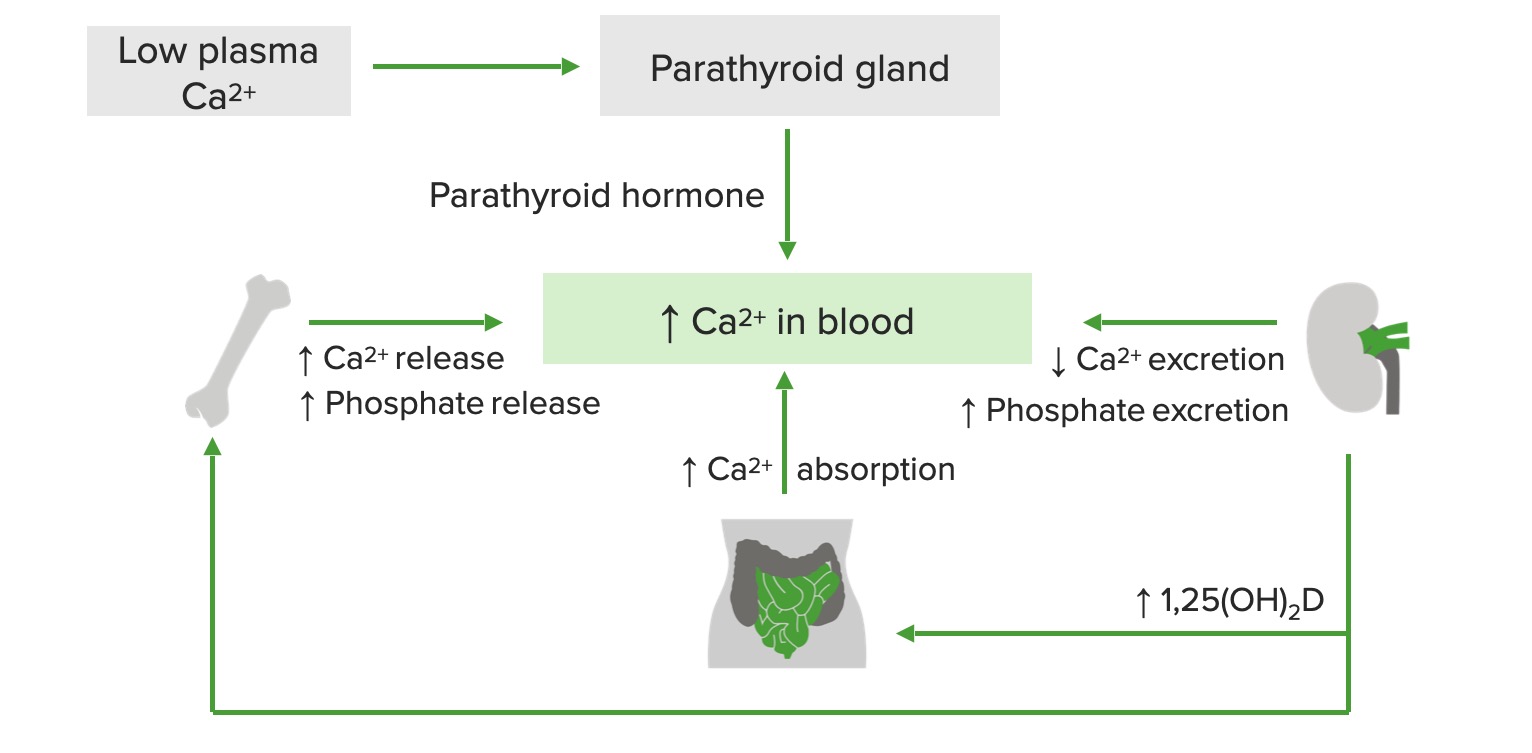
00:02 Now that we’ve looked at the overview of calcium homeostasis, let’s take a look at hypercalcemia and all the different pathologies associated with it. 00:11 Abnormal elevation of serum calcium, first step, workup is to confirm the elevation and always check to see as to what your free ionized calcium is because that would be the functioning form. 00:24 Calcium is 40 percent bound to albumin, it requires a chaperone. 00:28 Remember, overall calcium in-in the ECF is a very, very small percentage; 99 percent of your calcium is actually in your bone. 00:38 Remember that calcium and majority of it, in fact, is in ECF. 00:43 Therefore, any time a... any type of... any time there’s a channel that’s opened up for calcium, it will then rush in. 00:50 Adjusted total calcium, what does total mean to you? The bound plus the free or the ionized; always. 00:57 What is it that makes majority of your total? It’s the bound. 01:01 Adjust total calcium up to 0.8 milligrams per decilitre for every gram by which serum albumin is below 4 grams per decilitre. 01:13 Alkalosis increases calcium binding to albumin whereas acidosis decreases it and that’s an important point. 01:20 At some point in time, we’ll talk more about acidosis and the activity of osteoclasts and so forth, but at this point, understand that alkalosis increases calcium binding to albumin. 01:32 The more they’re positive, cation calcium will bind to albumin when there’s alkalosis state in your plasma. 01:42 Hypercalcemia acute, what kind of issues might the patient then have? Anorexia, nausea, vomiting, constipation. 01:49 CNS, there will be confusion and weakness, hyporeflexia versus tetany. 01:57 There is no muscle twitching in hypercalcemia, none; if anything hyporeflexia. 02:07 Cardiovascular, hypertension, shortened QT, not lengthened; occasional brady and maybe perhaps first degree AV block, you’re looking for prolonged, permanent prolongation of your PR interval. 02:26 In the kidney, maybe associated with polyuria, polydipsia, especially if you’re thinking about nephrogenic diabetes insipidus and prerenal azotemia, decreased filtration resulting in hypocalcemia. 02:42 These are issues that you’re looking for clinical manifestations of hypocalcemia. 02:49 Chronically, the pneumonic that you have probably come to become familiar with: stones, bones, groans and psychic overtones, pretty much tells you the problems that you would have with chronic hypercalcemia. 03:01 Stones, calcium stones, being the most common, calcium oxalate; bone issues groans, pain and psychic overtones; osteoporosis with bone pain, nephrocalcinosis with stones. 03:15 It will be band keratopathy, deposition of calcium-phosphate in sun-exposed cornea… keratopathy. 03:25 You have chondrocalcinosis, meaning to say that in the bone by the epiphyseal plate, you’d have accumulation of calcium... calcium, hypercalcemia may actually bring about damage to the pancreas. 03:40 You’ve heard of saponification and may cause hypertension.
About the Lecture
The lecture Hypercalcemia: Definition & Clinical Manifestation by Carlo Raj, MD is from the course Parathyroid Gland Disorders.
Included Quiz Questions
How does hypoalbuminemia affect calcium concentrations?
- Calcium is bound to albumin in the blood.
- Albumin controls intracellular concentrations of calcium.
- Albumin transports PTH.
- Calcium resorption is dependent on albumin concentration.
- Calcium is antagonized by albumin.
What is not seen in hypercalcemia?
- Areflexia
- Shortened QT interval
- Weakness
- Prerenal azotemia
- Nausea and vomiting
Author of lecture Hypercalcemia: Definition & Clinical Manifestation

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
