Playlist
Show Playlist
Hide Playlist
Coagulation Cascade

-
Slides NormalHemostasis.pdf
-
Download Lecture Overview
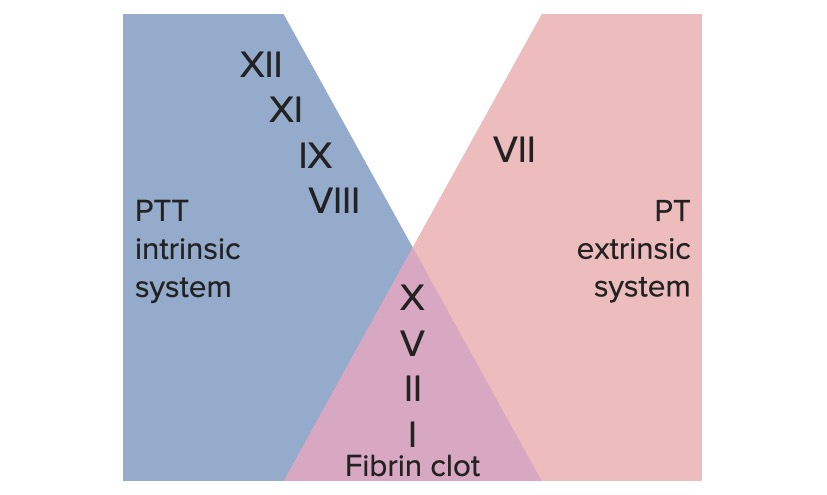
00:02 Here's the coagulation cascade. 00:04 I want you to first take a look at the overall picture and then we'll go into great detail. 00:09 As what it encompasses as you travel through coagulation cascade. Let's begin. 00:15 First you notice, I want you to first begin way down at the bottom here. 00:20 And you see where it says fibrin. 00:22 When was the last time we left or discussed fibrin or fibrinogen in the previous discussion? Oh, we had it with bound to, excuse me, what was the name of that receptor? I can't hear you. Yeah, that's it, glycoprotein 2b3a; that was the receptor that it was bound to earlier. 00:43 What was fibrinogen was? And I told you that we will then get in to discussion of coagulation cascade where we would take the thrombin and then cleave, notice now the cleavage of the fibrinogen into fibrin. 00:58 And now, with that fibrin, it would then form a clot that's much more stable versus temporary and then finally you must have factor XIII. 01:09 Factor XIII will then cause what's known as your cross-linking and make that clot incredibly, incredibly, well, stable and insoluble; that's the end game here. 01:22 With this you form a stable clot but let me put this into a big picture, right now, you and I, yeah, we formed that clot, fantastic. 01:32 But what if there was nothing to stop the clot formation? What if it continuously form thrombi, thrombi, thrombi? We would have problems, right? We can't have that. 01:42 So at some point in time not only are we going to form the thrombi but we're also going to do what? We're gonna break it down, aren't we? And it's all about homeostasis. It's like being on a see-saw. 01:52 In a see-saw, you can't have imbalance, in one is winning the battle at some point in time you must maintain homeostasis, so immediately there's also going to be the fibrinolytic system as we shall see cuz if you don't then you get into pathology. 02:07 Now that you understand where we are, where we're headed, above all of these, with thrombin, you'll notice that you'll take the letter X. 02:16 In Roman numeral X, it's the letter or number 10, isn't it? You take the X, you have the intrinsic over here and you have the extrinsic over here and you're gonna bring both branches on to and converge them on to factor X. 02:32 At this point, get a good bearing and get orientation of how the coagulation cascade works. All to do what? To cleave the fibrinogen into fibrin to form a stable clot; that's the overall picture here. Let's go into further detail and then later we'll revisit the coagulation cascade in greater detail. 02:57 Let's move. Let's take a look at that coagulation cascade in further detail. 03:03 Well, the initiation during the vascular phase of coagulation cascade is what tissue factor? And this will be part of what's known as your extrinsic system. 03:15 Now, ultimately that extrinsic system is then going to work upon and converge upon factor X. 03:21 Now with this occurring, a couple of things that you want to keep in mind, please, is that here we'll have factor VII with the extrinsic system as we shall see in the next picture. 03:32 Something else that you wanna keep in mind is that with the extrinsic system, let me add in some clinical medicine, if it's a extrinsic system then you should be thinking about measuring that extrinsic system via with something called prothrombin time. 03:48 In other words, PT, and then what PT really becomes important for you with is a drug called, warfarin. 03:57 And are you beginning to understand as to why all this is important? We initiate the extrinsic system via the tissue factor and then with this ultimately we're going to take that fibrinogen by activating the thrombin in making it into a fibrin polymer and we have a stable clot. 04:17 Let's take a look at that extrinsic system over on your left, please. 04:23 Take a look at where we begin, and I need you to memorize factor VII, however you do so, please do so. 04:28 Factor VII begins the extrinsic system. 04:32 Earlier I told you that the lab value that you're gonna use or the labs that you'll be using would be PT. 04:38 You memorize the following and I'll repeat this over and over again. 04:42 The PT time is approximately 11 to 13 seconds and it is often standardized to an International Normalize Ratio or INR, by dividing the patient's PT, by a reference control PT to correct for different analyzers and reagents used. 04:58 An INR of 1.0 is normal. 05:01 If this is the first time that you're hearing it, get use to it. 05:06 I'll keep repeating it until it becomes part of your subconscious reflex. 05:10 Next, with the extrinsic system, what's the drug that primarily works via extrinsic system? It would be heparin or warfarin. 05:20 So in a little bit, we'll have a discussion, a very important discussion to make sure that we delineate the differences between warfarin and heparin; warfarin and heparin. 05:31 We would begin by talking about warfarin. 05:34 Warfarin works on what's known as your vitamin K dependent factors. 05:39 These vitamin K dependent factors, you group this into four on one side and two in the other for a total of six. 05:48 What do you mean four on one side and two in the other? Remember, it's all about maintaining homeostasis. 05:53 Remember that see-saw that I was talking to you about? You can't be on one side of the see-saw for too long or otherwise you would then go into pathology. 06:02 So what is it that brings the see-saw back to its normal or create a balance? The other two factors which include protein C and protein S. 06:12 So, all of these, will work via your extrinsic system. 06:17 All of these will be playing a role as we shall see with warfarin, which is vitamin K dependent factors and later on are going to much greater detail. 06:28 You'll notice that factor VII here converges upon factor X and then from factor X, what was the name of that "omnipotent enzyme" responsible for cleaving your fibrinogen? Oh, it's called thrombin. 06:43 You take the T in thrombin, please, and you must know that thrombin is factor II, T-W-O, T and T. 06:52 That's important, isn't it? Extremely. 06:55 Later on, we'll have a discussion about management and I'll ask you about a drug that works through antithrombin III and that would be heparin, that would be heparin. 07:09 Or I'll introduce you to new drugs called dabigatran or argatroban and these are direct acting thrombin inhibitors. 07:20 Are we okay so far? Now, for the first time, let's take a look at the intrinsic system. 07:29 Now I'm going very methodically here because I wanna make sure that I'm very clear about how you should be approaching the coagulation cascade. 07:38 Under the extrinsic system you need to memorize that it begins with factor XII and that the name for factor XII is Hageman factor. 07:47 Now I'm gonna stop here for one second because I don't want you to glaze over some important points that you see here on the far right. 07:55 On the far right, earlier, I told you, I've mentioned this a few times in one of my favorite analogy's is about maintaining homeostasis via see-saw. 08:06 So, on a see-saw ones again, remember, factor XII, if it had its own way, if nothing was stopping it, you would have unrestricted thrombi formation, correct? But you and I, not only do we develop a thrombi, we also have to have a system where it's breaking it down and we call this, the fibrinolytic system. 08:27 The "enzyme" they're primarily responsible for fibrinolysis -- take a look at the far right -- is plasmin. 08:37 So what factor XII will do once a thrombi has been formed is to make sure that it also puts on the breaks. 08:45 It puts on the breaks and keeps things in balance by activating plasmin. 08:51 So now, we have three components in the coagulation factor that sounds very, very similar that you need to make sure that you take a moment and you digest and understand the proper use of each one that included fibrin which is going to form your stable clot. 09:10 What cleaved the fibrinogen to form fibrin? That was thrombin. 09:15 Thrombin and fibrin are both going to promote coagulation, is that clear? And then on the other side, meaning, what's going to breakdown your clot or your fibrinolytic component would then be what? Plasmin. Are we okay so far? If not, make sure that you take a moment and you're clear about those three components of your coagulation cascade. 09:41 And then after factor XII, you have factor XI, and your factor IX, let's come down to factor VIII and spend a moment on factor VIII, please. 09:49 Now before I move on with the intrinsic system, what is the laboratory test that you're gonna use here? This is called PTT. What is it for the extrinsic system? PT. 10:02 Would you remind me again what, what the time was for PT? 11 to 13 seconds. 10:09 Now when you add a T, PTT, you add more time. 10:16 The normal PTT time which stands for Partial Thromboplastin Time, is going to be between 25-40 seconds. 10:25 Now each one of these I'm gonna keep repeating over and over again but I need you to spend some time on the times and the different components of your coagulation cascade. 10:36 Next, I want you to take a look at a particular factor here, it's called PF3 and that also would play a role with stabilization of not only factor VIII but then will converge upon what factor here? There is factor X. 10:51 I need you to know that factor X in Roman numeral is going to be the letter X, for two important reasons. 10:58 Early I told you to take the X, this branch over here will be the intrinsic, this one over here will be extrinsic, right? Both of these will converge upon factor X. 11:07 We'll take the X and then later on I'm gonna give you some new drugs that you need to know. 11:11 These drugs that inhibit factor X will then be called apixaban or rivaroxaban, okay? So whenever you see that letter X, you should be thinking about factor X. 11:24 Now with this, you form a prothrombin complex cuz what you're gonna do? You're gonna finally activate that thrombin. 11:29 Remind me again what that factor is for thrombin? Take the T in thrombin, its factor II. 11:35 Why did you wanna know that again? Because you've talked about heparin, and we will talk about heparin again and with heparin it works via antithrombin III or your drugs such as dabigatran or argatroban that are direct acting thrombin inhibitors. 11:51 We spend some time here in coagulation cascade; let's spend a little bit more time moving forward delineating or elaborating on some of the details here. 12:02 You notice the vitamin K dependent factors. 12:06 There are four of them that are procoagulant. 12:10 Remember I told you vitamin K dependent factors you divide them into two components. 12:14 You have the procoagulants -- factor II, VII, IX, and X. 12:17 Memorize that, II, VII, IX, and X. 12:20 What organ are you thinking automatically when you talked about vitamin K dependent factors? Liver, right? So here in the liver these undergo something called gamma carboxylation. 12:31 So these are gamma carboxylated components. Who helps with this? Or, well, the vitamin K obviously plays a role, calcium will play a role and then warfarin is going to be a drug that inhibits vitamin K dependent factors. 12:45 Now these are the four that are procoagulant. 12:47 Remind me again, what we're the two that were anticoagulants? Later on we'll talk about protein C and S. 12:53 Big picture -- all the vitamin K dependent factors, there are six of them, II, VII, IX, and X, protein C and protein S for a total of six. Is that clear? Next, there's something else that I need you to understand. 13:09 There's an enzyme here that helps you with the gamma carboxylation, it's called epoxide reductase. 13:15 I'll repeat that again, it's called epoxide reductase. 13:19 It is important that you know that because now we know further detail molecularly with warfarin as we should talk because not at all times could warfarin be let's say effective in all patients and the reason for that is you might have polymorphisms in those vitamin K dependent factors specifically with the epoxide reductase as we shall see.
About the Lecture
The lecture Coagulation Cascade by Carlo Raj, MD is from the course Hemostasis: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following is released from fibrinogen through the action of thrombin?
- Fibrinopeptides A and B
- Soluble fibrin
- Prothrombin
- Tissue thromboplastin
- Plasminogen
Which coagulation factor completes the cross-linking of fibrin for mesh formation?
- XIII
- VIII
- VII
- V
- XI
Which of the following factors plays an essential role in the initiation of the extrinsic pathway of coagulation by binding to factor VIIa?
- Tissue factor
- Factor XIII
- Factor VIII
- Factor X
- Plasminogen
Prothrombin time is a measure of which of the following components of the coagulation cascade?
- Extrinsic pathway and common pathway
- Common pathway and intrinsic pathway
- Extrinsic pathway and intrinsic pathway
- Intrinsic pathway only
- Common pathway only
Which of the following values represents the normal range for the international normalized ratio (INR)?
- 0.8-1.1
- 15—19
- 1.5-2
- 2.5-2.8
- 1.2-1.5
Which clotting factor is responsible for transforming prothrombin into thrombin?
- Factor X
- Factor XIII
- Factor VIII
- Tissue factor
- Fibrinogen
Author of lecture Coagulation Cascade

Carlo Raj, MD
Customer reviews
3,4 of 5 stars
| 5 Stars |
|
3 |
| 4 Stars |
|
2 |
| 3 Stars |
|
0 |
| 2 Stars |
|
1 |
| 1 Star |
|
2 |
Very, very nice, thanks a lot for the big help doctor
Very interesting way to explain this subject!!!!!! Thank you so much
Dr Raj is both serious and funny at thesame time. I love it when he does 'hmm'. Fantastic teacher!
I decided to rate this lecture as a 1 because of the confusing diagram. If the diagram would have been broken down it might have been better to learn from. But having the entire diagram of extrinsic and intrinsic pathways completely filled out at once made it incredibly difficult to follow along. I felt like it was unclear and jumped around a bit.
