Playlist
Show Playlist
Hide Playlist
Abdominal Pain: Examination

-
Emergency Medicine Bord Approach to Abdominal Pain.pdf
-
Download Lecture Overview
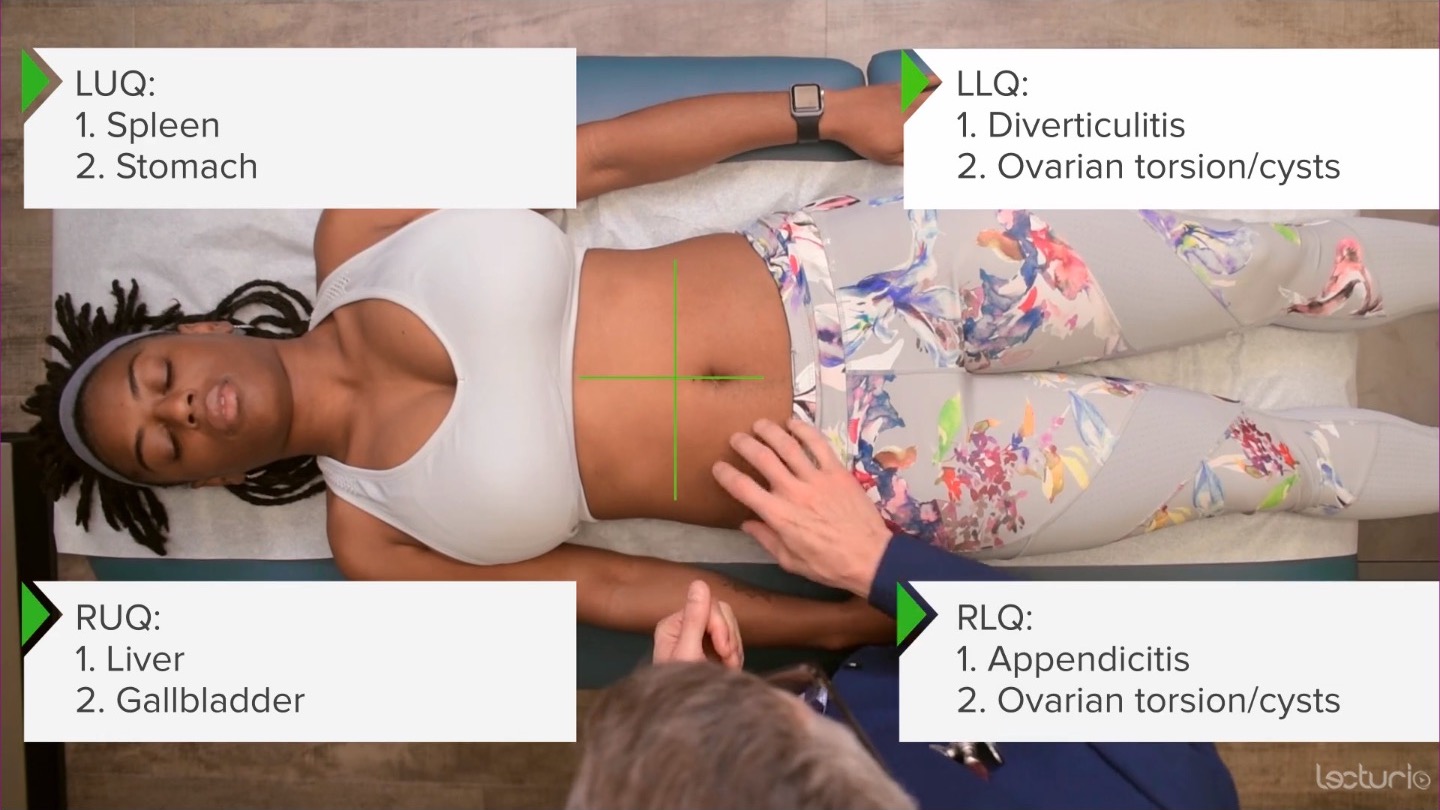
00:01 So in the exam we wanna go through a few steps. 00:04 So step one in the physical exam is the vital signs. 00:07 Vitals are vital. 00:09 You probably have heard me say that if you’ve listened to some of these other lectures. 00:12 You wanna make sure you have a full set of vital signs on your patient. 00:16 Sometimes it can be easy that one of them maybe overlooked a little bit but definitely having an accurate temperature reading, a blood pressure reading, a pulse oximeter, a heart rate and a respiratory rate. 00:28 All will benefit you in this situation and you wanna make sure you're paying attention to all of those vital signs. 00:34 Step two is to inspect. 00:37 So is the patient laying still or are they restless? Are there any prior surgical scars on their abdomen? Similar to when a patient comes in with a respiratory distress, there's a lot of information you can get just by looking at your patient. 00:51 If they’re laying still that can potentially indicated they have peritoneal signs. 00:56 Them moving around might make their pain a little bit worse. 00:59 If the patient is restless, that might support renal colic, or a kidney stone diagnosis classically those patient are very restless. 01:07 Some patients also aren’t very good at remembering what procedures they’ve had on their abdomen and some patients might, you might ask them I’ve had the situation for sure, “Have you ever had any surgeries on your abdomen?” And they say no and then you look at their belly and there’s lots of scars there. 01:25 So in those situations you wanna go ahead and maybe ask some of a little bit more approving details. 01:30 If you see surgical scars or look in the medical record to try and figure out what happened. 01:35 Surgical scars are becoming harder and harder to necessarily notice especially with more and more people getting laparoscopic surgery. 01:43 Cause those laparoscopic surgical scars are very very small and are often try to do them in less noticeable areas. 01:50 So one classic places are just around the umbilicus and those can be a little bit harder to pick up on. 01:56 Step three is to listen. 01:59 Historically, everyone’s taught to listen before you palpate. 02:02 So go ahead and go with that for now. 02:04 You wanna listen for two minutes and you're listening for bowel sounds. 02:08 If you don't hear any bowel sounds after a full two minutes, the patient does not have bowel sounds likely. 02:14 So, you wanna make sure you're listening for that appropriate time period and you’re hearing if the bowel sounds are overactive, underactive, not present at all, or potentially in the normal range. 02:26 Step four is palpation. 02:27 You wanna start in the area away from the pain. 02:30 So if the patient's pain is on the right side in the lower abdomen, go ahead and start on the left upper abdomen and then work your way around to that area. 02:38 You’re gonna wanna palpate lightly and then go ahead and push a little bit more deeply depending on the exam that you’re getting for the patient. 02:46 When you're palpating you also wanna go ahead and access for rebound tenderness. 02:51 So rebound tenderness is basically pain that occurs when you let go. 02:55 So basically you push down on the abdomen and when you release your hand, I tell people to try and focus does it hurt more when I push down? Or does it hurt more when I let go? Rebound tenderness is potentially supportive of the patient more likely having a surgical process. 03:11 The other things you can do to access for rebound tenderness is that you can sometimes shake the bed. 03:16 This was a tip that I learned actually when I was a medical student from one of my surgery residents. 03:20 And he would go to rooms for patients that were being worked up. 03:23 And he would basically take his knee and he would nudges the bed a little bit and see if the patient reacted. 03:29 Shaking of the bed reproducing abdominal pain is again, something that indicates that the patient may have peritoneal irritation and possibly a surgical process. 03:40 The other thing that you can do and this is more commonly done in the pediatric population is you can get your patient up out of bed and you can have them jump on one foot. 03:47 Again, that’s something that indicates that if they have pain that’s reproduced in that situation, then the patient may have more likely to have appendicitis or a surgical process. 03:57 This is a classic thing in pediatrics that they get their patient up and have them jump on one foot and if the kid’s willing to or able to do it without pain, a lot of pediatric ED people will say that the likelihood of appendicitis is far less likely. 04:11 The other thing that I do sometimes ask patients is I have them estimate when they came to the emergency department in their car, if going over bumps bother them. 04:20 Again, it's an element of just that little shaking movement or vibrations causing or making that pain worse. 04:28 There are some additional exam maneuvers that you wanna think about doing. 04:34 So one of them is Murphy’s sign and that is taking a closer look at the gallbladder kind of indicating if there is a disease in the gallbladder for cholecystitis, and what you do in that situation is you feel in the right upper quadrant and when you're palpitating deeply in the right upper quadrant the patient stops inspiring and that’s indicating that that pain is so severe or intense or localized to that area that the patient will stop inspiring. 05:01 This is something that can be done on physical exam and also can be done during an ultrasound exam. 05:07 So when you’re doing the ultrasound for the patient, you can see if they have a positive Murphy’s. 05:14 The other thing you can do and this is generally done in the center of the abdomen is you can palpate the aorta. 05:19 You wanna think about AAA in older patients. 05:23 So as patients are older is when this disease process generally does start to develop. 05:28 So for those patients you wanna go ahead and feel the center of the belly and see if you feel any kind of larger palpable mass. 05:34 In skinny younger people you actually maybe able to feel their aorta because they're generally skinny and younger, and you’re able to feel it in the center of their abdomen. 05:46 Other maneuvers are the psoas, obturator, and Rovsing's sign. 05:50 Those are indicative of appendicitis and we’ll talk more about those when we discuss appendicitis further. 05:57 The other things to focus on are genitourinary exams, the testicular exam and the pelvic exam. 06:03 The testicular exam is especially important for the patient who your concern may not necessarily be able to accurately report to you whether or not they are having testicular pain. 06:14 The pelvic exam I always tell women when they come to the ED with abdominal pain that they're really quite tricky because in addition to having your intestines and the normal stuff in your belly you also have your reproductive organs. 06:27 So you have the uterus and ovaries and those are sometimes the source of the pain. 06:32 So doing a pelvic exam for all women who have uterus and ovaries is a key thing to do when they present with abdominal pain because you don't wanna miss the pelvic infection or some kind of ovarian mass that's presenting in that way. 06:49 You also wanna look for any kind of extra abdominal findings. 06:52 So that means that the herpes zoster rash that was discussed. 06:55 It means listening to the patient’s lungs and seeing if there's any concern for pneumonia. 07:00 Looking at the respiratory rate and seeing if the respiratory rate is elevated, that might make you support on diabetic ketoacidosis. 07:07 If you're worried about glaucoma, examining the face and eyes.
About the Lecture
The lecture Abdominal Pain: Examination by Sharon Bord, MD is from the course Abdominal and Genitourinary Emergencies.
Included Quiz Questions
What is the first step in the examination of a patient with abdominal pain?
- Vital sign assessment
- Abdominal inspection
- Auscultation of bowel sounds
- Palpation of the abdominal area
- Determine presence of rebound tenderness
What is the appropriate duration of auscultation in the assessment of the bowel sounds?
- 2 minutes
- 15 seconds
- 30 seconds
- 45 seconds
- 1 minute
What is the most likely diagnosis in a patient with a positive Murphy’s sign?
- Cholecystitis
- Pancreatitis
- GERD
- Viral gastroenteritis
- Lower lobe pneumonia
Author of lecture Abdominal Pain: Examination

Sharon Bord, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
