Playlist
Show Playlist
Hide Playlist
Carpal Tunnel Syndrome: Management

-
Slides Carpal tunnel Special Surgery.pdf
-
Download Lecture Overview
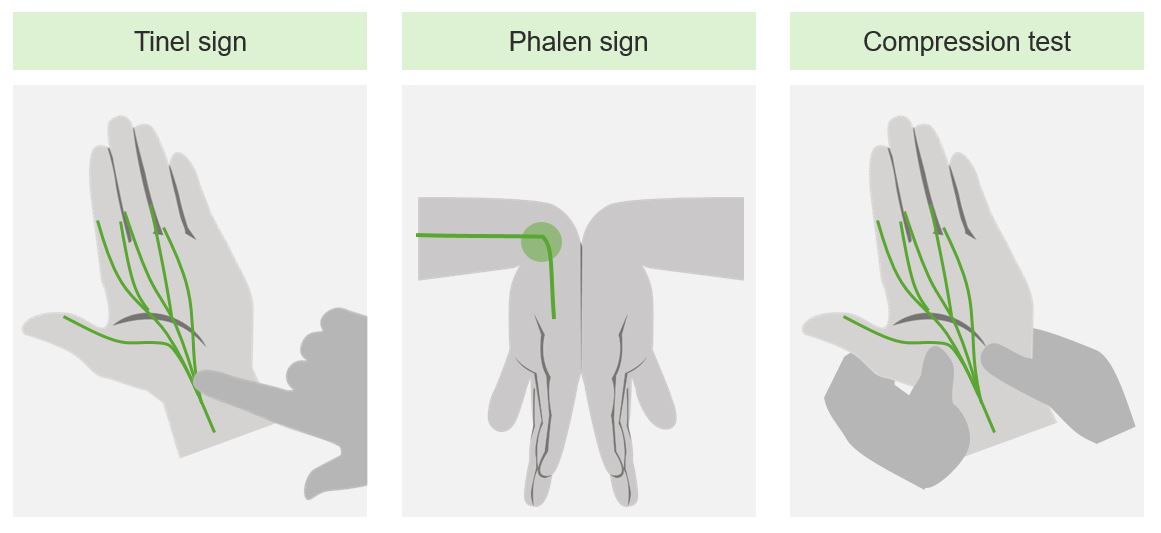
00:01 How do we manage carpal tunnel syndrome? Medically, we offer occupational and physical therapy. 00:10 Wrist splinting to a neutral position may be helpful. 00:14 Remember those wrist rests that people use on keyboards. 00:18 It’s partly to try to reduce the incidence of carpal tunnel syndrome. 00:22 Sometimes, steroid is injected into the region for symptomatic relief If necessary, or the clinical symptoms deteriorate, we can offer surgery. 00:35 This is usually for the patients who have severe carpal tunnel syndrome. 00:39 Severe carpal tunnel syndrome can be described by EMG (or electromyographs). 00:47 Here, we evaluate the actual conduction of the nerve and whether or not there's truly compression of the median nerve. 00:54 We release the transverse ligament, allowing the carpal tunnel syndrome to relieve in terms of symptoms, but it may not be as helpful if the previous EMG demonstrates that there was now full compression of the median nerve. 01:10 Here's that demonstration of the EMG. 01:13 Multiple electrodes are placed over the distributions of the median and radial nerves. 01:20 Here's a picture of a transverse ligament release. 01:23 Note the palmar area is exposed surgically. 01:28 With full release of the transverse ligament, the median nerve should no longer be compressed. 01:32 Symptomatic relief is usually fairly immediate. 01:40 Now, let's visit some important clinical pearls and high-yield information. 01:45 Individually, each of the classic physical signs has low sensitivity and specificity for carpal tunnel. 01:51 As a unit, it’s usually highly diagnostic. 01:55 Remember the classic presentation and don't forget the distribution of the median nerve. 02:03 Sensory loss with median nerve impingement, again, to remind you include palmar aspects of digits one, two and three and the radial half of the fourth digit. 02:12 Thank you for joining me in this discussion of carpal tunnel syndrome.
About the Lecture
The lecture Carpal Tunnel Syndrome: Management by Kevin Pei, MD is from the course Special Surgery.
Included Quiz Questions
A patient presents to you with mild carpal tunnel syndrome. What is your first step in management?
- Wrist splinting at night
- Endoscopic transverse ligament release
- NSAIDs
- Steroid injections
- Open transverse ligament release
Symptoms of carpal tunnel classically occur in which of the following digits?
- Palmar aspect of digits 1, 2, 3 and the radial half of the 4th digit
- Palmar aspect of digits 2, 3, 4 and the radial half of the thumb
- Palmar aspect of digits 2, 3 and the radial half of the 4th digit
- Palmar aspect of digits 1, 2, and the radial half of the 3rd digit
- Palmar aspect of digits 1, 2, 3, 4 and the radial half of the 5th digit
Author of lecture Carpal Tunnel Syndrome: Management

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
The class is good, very easy to learn in short time.
