Playlist
Show Playlist
Hide Playlist
Disorders of Carbohydrate Metabolism

-
Slides MetabolicDisorders Pediatrics.pdf
-
Download Lecture Overview
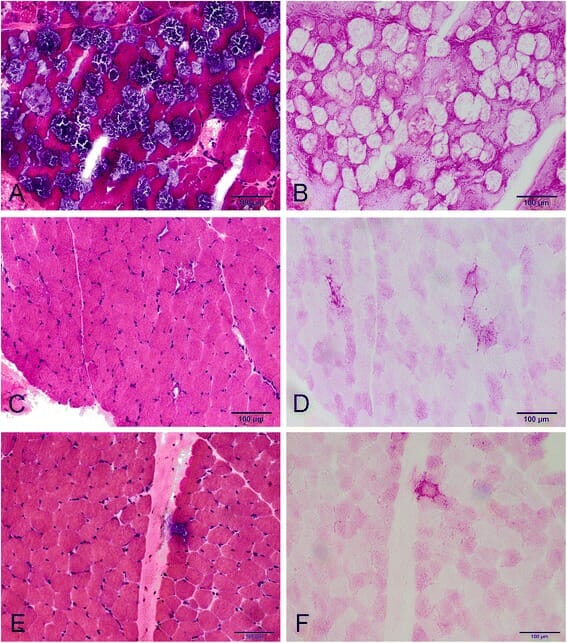
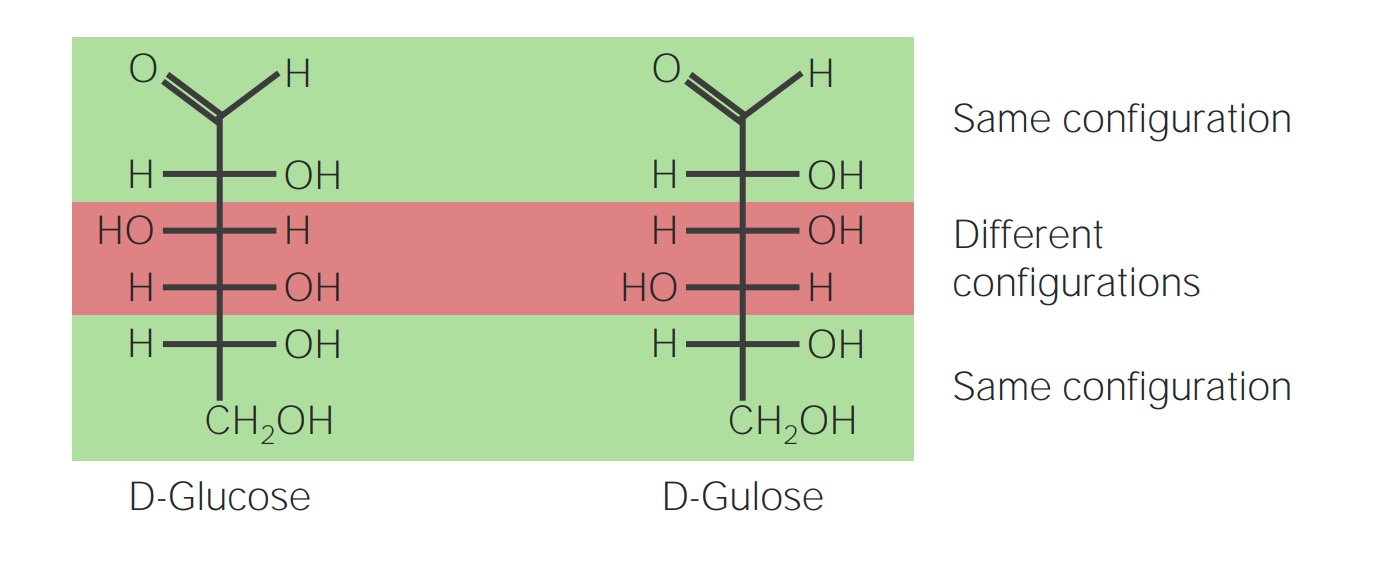
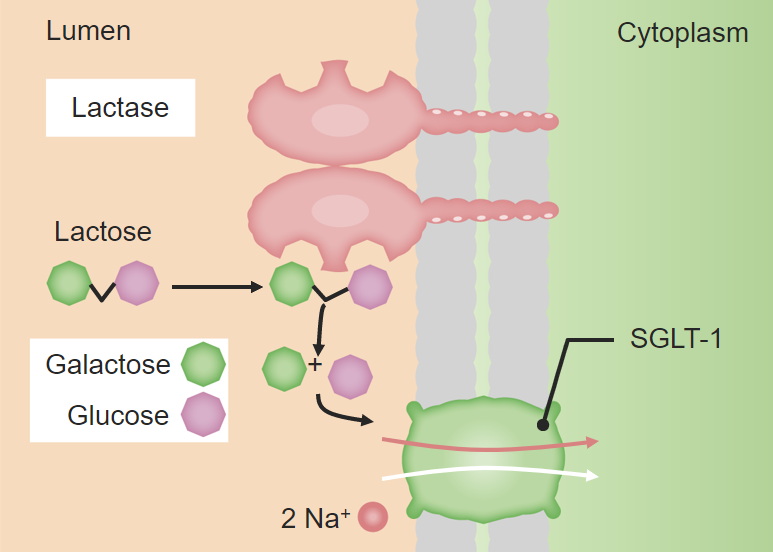
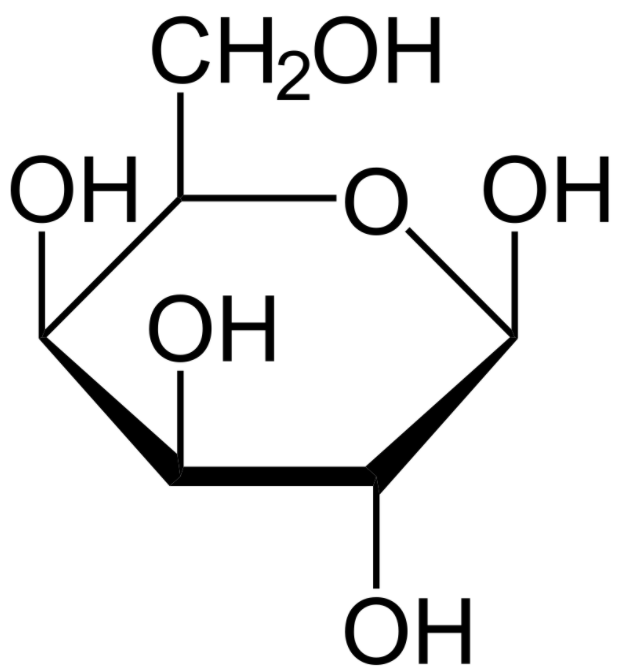
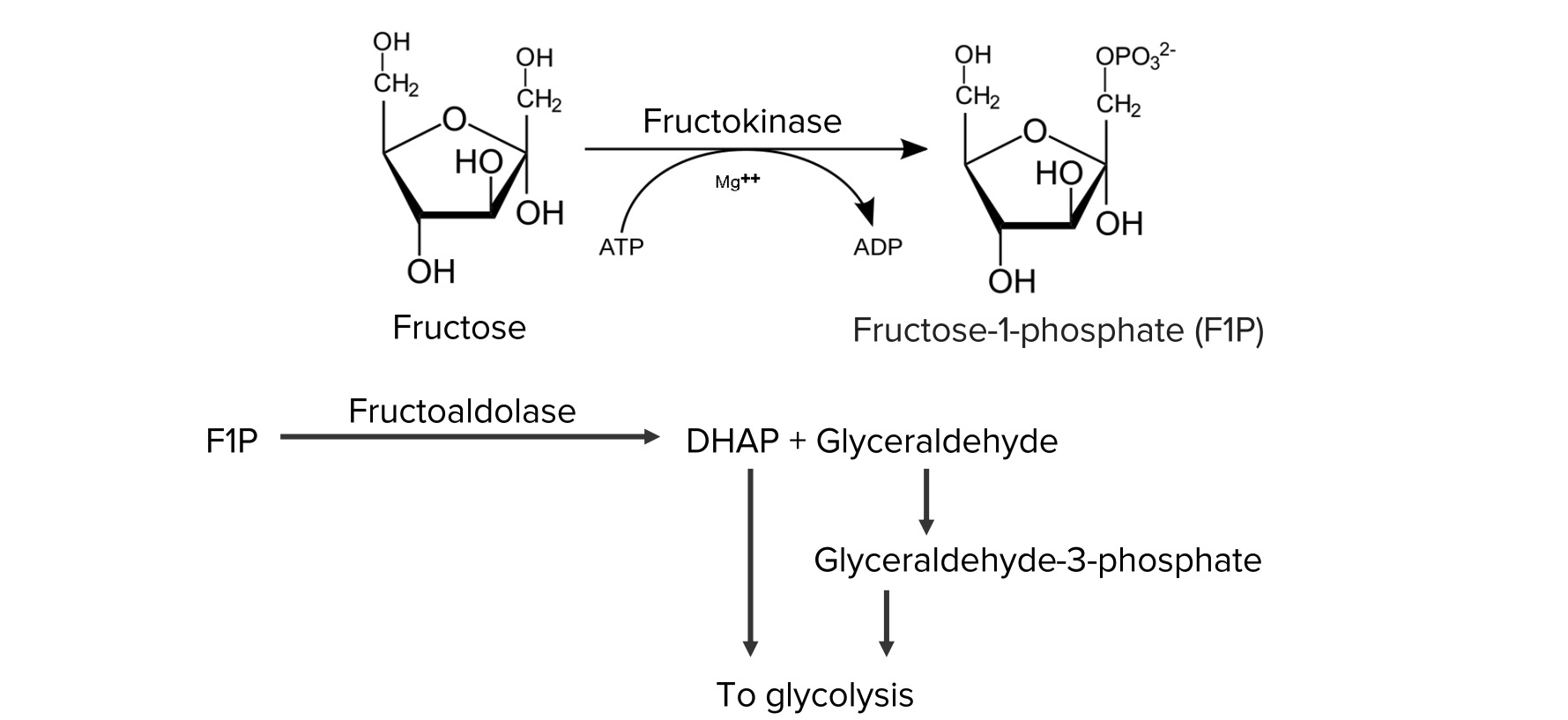
00:01 Let's start with disorders of carbohydrate metabolism. 00:05 We can see patients with problems in glucose metabolism, fructose metabolism, and galactose metabolism. 00:14 I've drawn here the galactose differently than glucose because the OH group goes off in a different direction. 00:20 It's a cartoon but I think it's effective. 00:23 Glycogen storage diseases are probably the most common issue around glucose metabolism. 00:29 Essentially, enzyme defects in glycogen breakdown result in an inability to make glucose after a short period of fasting in the liver and the muscle. 00:42 So patients can present with both hepatic disease and muscle disease. 00:46 In other words, they're having a problem getting the glucose out of their glycogen stores. 00:52 With hepatic disease, a short fast can cause hypoglycemia. 00:58 It usually shows up in the first 6 months of life as children start to space out their feeds. 01:05 Typically, a newborn baby is eating every 2 hours, the glycogen storage aren't that important. 01:10 As they get older, they rely on their glycogen storage more because they're going longer distances between feeds. 01:17 These patients can present with muscle weakness and they can present with hepatic cirrhosis at times. 01:24 The muscle disease is a progressive muscle weakness and sometimes can involve the heart as well. 01:31 And in some varieties of glycogen storage diseases, the cardiomyopathy is the most important thing. 01:38 Any child with cardiomyopathy is primarily gonna present with fatigue. 01:42 Let's go through three really common glycogen storage diseases. 01:48 The first one is Von Gierke's disease. 01:51 And I like to think about Von Gierke's as primarily in the liver. 01:56 This is also glycogen storage disease type 1. 01:59 These patients will present with a profoundly challenging hypoglycemia. 02:04 They will have hepatomegaly from their liver involvement. 02:07 They will develop hyperlipidemia as well. 02:10 Because of their underlying problem, they may have growth failure but they will not primarily have weakness. 02:17 Most of their diseases related to the liver. 02:20 That's as opposed to Pompe's disease. 02:24 Pompe's disease can be very severe in childhood or it can develop later. 02:30 But this is glycogen storage disease type 2 and it's primarily involving the heart. 02:36 They do not develop hypoglycemia. 02:39 They still do get some hepatomegaly but it can either be very severe with a inevitable death by the age of 2 or can be more benign. 02:51 Clearly, a heart failure is the most important heralding symptom of Pompe's disease. 02:56 The last example would be McArdle's and when I think of McArdle's I think of muscle. 03:02 Muscle McArdle's. 03:03 This is glycogen storage disease type 5. 03:07 It really only has muscle involvement, so these patients develop the weakness but not as much of the other symptoms. 03:15 They may develop renal problems from myoglobin breakdown and sledging in the kidney causing renal damage, so monitoring for that is important. 03:25 Let's switch to another type of sugar which is galactosemia. 03:31 Remember that galactose is metabolized through a pathway involving two major enzymes. 03:38 Galactose is turned into galactose 1 phosphate through galactokinase. 03:44 Galactose 1 phosphate has that enzyme GALT which then turns it into glucose 1 phosphate and then we can metabolize the galactose. 03:53 Remember that the galactose, the sugar in milk, is a galactose plus a glucose stocked together. 04:00 Lactase breaks those apart and then for the galactose, we use this pathway to metabolize it. 04:06 In patients with galactosemia, they have a defect in one of these two enzymes. 04:11 Galactokinase deficiency is very rare, we almost never see it. 04:17 Those children typically have a milder course. 04:20 But GALT deficiency is not too uncommon, and we do see periodically patients with GALT deficiency. 04:27 GALT deficiency usually presents once milk is introduced. 04:33 As you can imagine, milk is introduced essentially right at birth. 04:37 So we screen for galactosemia in the newborn screen so that we can prohibit the child from getting milk once they're born if they have this problem. 04:49 We need to give them a special formula that does not have galactose in it. 04:55 Patients where they are not picked up will develop failure to gain weight, vomiting, lethargy, jaundice, hypoglycemia, and this is key for your exam, cataracts. 05:09 Exams love to mention cataracts. 05:11 These children can also develop renal failure. 05:14 So obviously, screening for these diseases is very important. 05:18 Even if effectively picked up on the newborn screen and a rapid intervention is made, these children can still have problems over time. 05:28 They can develop speech delay, ataxia, gonadal failure, problems can happen. 05:33 But their course is much better if we can make a dietary intervention early in life. 05:38 Very rare, but we can see hereditary fructose intolerance as well. 05:44 This generally presents once fruit is introduced. 05:47 These children can't metabolize fructose well. 05:50 They generally would develop an increased pyruvate and lactate which leads to a metabolic acidosis. 05:57 These children can develop abdominal pain, nausea, vomiting. 06:00 They can have a severe hypoglycemia as well, which ironically, is not relieved by a fruit juice. 06:06 They can develop lethargy, seizure, and diarrhea. 06:11 So these children really need to avoid fructose in their diet.
About the Lecture
The lecture Disorders of Carbohydrate Metabolism by Brian Alverson, MD is from the course Pediatric Endocrinology.
Included Quiz Questions
A patient presents with generalized weakness and myoglobinuria but has a normal glucose level. The patient is found to have a glycogen storage disease. What is the most likely diagnosis?
- McArdle’s disease
- Pompe’s disease
- Von Gierke’s disease
- Cori’s disease
- Forbes’ disease
A 2-year-old child is brought to the ER with severe fatigue. On examination, she has hepatomegaly. An immediate echocardiogram is suggestive of heart failure. You suspect glycogen storage disease and decide to do some lab tests. Which of the following is the most likely cause?
- Pompe disease
- Cori’s disease
- Forbes’ disease
- McArdle’s disease
- Von Gierke’s disease
A 12-year-old boy is brought to the ER during a hypoglycemic episode. His parents say that he has had this kind of episode in the past. His glucose level is corrected. As you examine the patient, you notice hepatomegaly, and his height and weight are both 25th percentile for his age. Lab reports show hyperlipidemia. Which of the is the most likely cause of his symptoms?
- Von Gierke’s disease
- Pompe’s disease
- McArdle’s disease
- Forbes’ disease
- MCAD deficiency
You suspect that a child has galactosemia. Which of the following is a clinical feature unique to this disease?
- Cataract
- Failure to gain weight
- Lethargy
- Jaundice
- Hypoglycemia
Author of lecture Disorders of Carbohydrate Metabolism

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
3 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent lecture, very clear and well explained. Thank you so much!
Excellent lecture. This is a difficult topic and it was made very clear, especially the mnemonics.
Very clear lecture right on points. Thank you for making complicated concepts straight forward.
