Playlist
Show Playlist
Hide Playlist
Pediatric Iron Deficiency Anemia, Vitamin B12 Deficiency, Folate Deficiency & Erythrocyte Aplasia

-
Slides Anemia Alverson.pdf
-
Download Lecture Overview
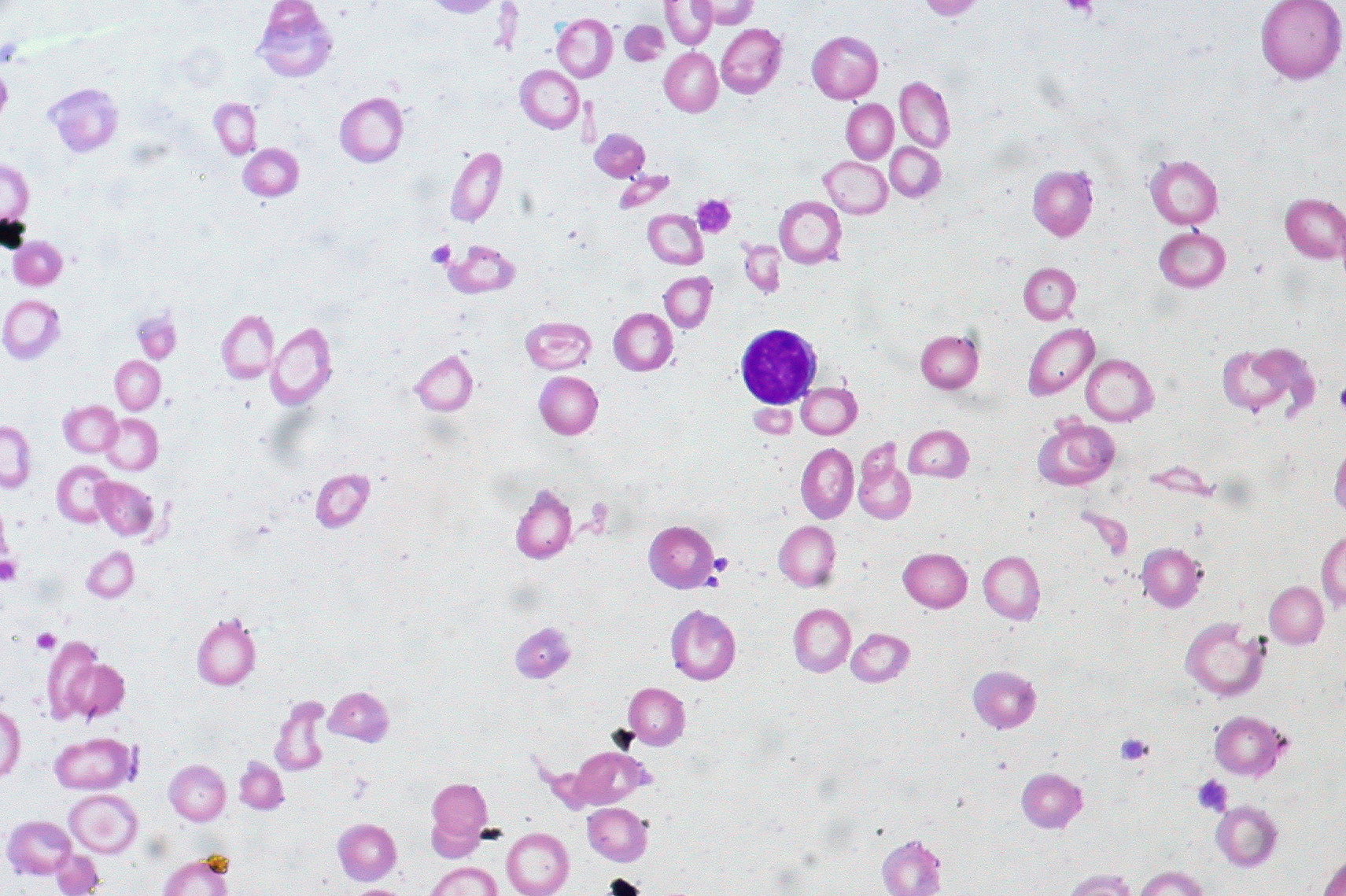
00:01 So let’s focus on iron deficiency anemia and I want to do that because this is so common in children. 00:08 This is more common in periods of rapid growth, when kids need their iron the most. 00:14 Also, it’s more common on strict vegetarians because iron is repleted in meat. 00:19 Most commonly, we see it in infants who drink lots of milk. 00:23 I’ve had many patients come in and mom says, “Oh, that’s the only thing he’ll eat and I want him to grow and so I give him 4 glasses of 8 ounces of milk a day.” Those children are going to present with anemia. 00:36 Occasionally, iron deficiency can also be seen in blood loss because when you lose blood, you’re essentially losing iron if you don’t replete the iron in your diet. 00:45 So patient’s with inflammatory bowel disease, GI bleeds or parasites, celiac disease or even patients with excessive menses are all at risk for iron deficiency. 00:57 Well in adolescent girls, even girls with normal menstrual issues can have blood loss and resulting iron deficiency if they are not having enough iron in their diet. 01:08 So for iron deficiency, the CBC will show a microcytic anemia and they will typically have a low erythrocyte count. 01:17 You might want to get iron studies. 01:19 Sometimes, I get confused about the iron studies so let’s go through them carefully. 01:23 So, the ferritin reflects your total body stores. 01:28 This is the best single test for iron deficiency and it usually is low in iron deficiency because this is reflecting your body stores of iron. 01:37 The challenge with ferritin is it's also an acute phase reactant. 01:41 So if I get a pneumonia, I’m going to have a high ferritin. 01:44 I may have iron deficiency and have a falsely high ferritin and miss the diagnosis if ferritin is the only thing I’m getting. 01:51 Another iron study you might get in your iron panel is the total iron-binding capacity. 01:57 This represents how many free transferrin sites there are in a patient. 02:02 So if there are lot of free spaces for iron to bind, that means your iron is low, they should be bound, they are not, so you may have a total iron binding capacity this high. 02:13 If I have a patient who has inflammation and a normal ferritin and a high iron binding capacity, I may have a patient with iron deficiency, oh yes, and their ferritin is high because they have a pneumonia. 02:26 The serum iron is not really a particularly useful test. 02:29 It comes along with that often. 02:31 I don’t use it very often. 02:34 So how do we manage iron deficiency anemia? It seems pretty obvious we have to give them iron. 02:39 Usually, we provide iron as a medication, a dose of around 4-6 mEq/kg/day. 02:46 We’re going to restrict milk consumption in these children because that is such a common cause. 02:51 Sometimes kids don’t want to go along with that plan and you have to spend some time encouraging the families to teach them how to say no to their child who wants more milk. 03:00 Additionally, we will hopefully increase iron-containing foods. 03:04 You can look that up on the internet, involves foods like meat and legumes. 03:09 We often supplement vitamin C because this facilitates iron absorption in the gut. 03:15 Also, if a patient has become tachycardic, we’re going to need to transfuse that patient. 03:22 Typically, this is at hemoglobin of around 7. 03:26 We don’t usually use the hemoglobin number itself for when we need to transfuse, we usually use when they’re tachycardic. 03:34 However, you may use it in certain circumstances. 03:37 An example would be if a patient has a brisk GI bleed and was 9 and then was 7 and still is tachycardic, I’m probably going to transfuse that child because next time I look, the child will be 5. 03:52 Okay, vitamin B12 and folate deficiency. 03:55 This is much more common in adults than children because B12 and folate are fairly ubiquitous in the diet. 04:04 We typically think of this as a problem in adult alcoholics. 04:08 It could happen in a very severe teen alcoholic, but whatever the case may be deficiency of these two nutritional elements cause a macrocytic megaloblastic anemia. 04:21 B12 is absorbed in the ileum, so we also see this problem in patients with ileal inflammation. 04:30 The classic example would be a Crohn’s patient. 04:34 Nutritional deficiency like I said is rare. 04:37 We will treat these patients with IM vitamin B12. 04:42 Folate disease is very, very rare in children and generally associated with a generalized malnutrition. 04:50 We use oral supplementation of folate and that will be fine. 04:54 So both of these are erythrocyte aplasias. 04:59 Transient erythroblastopenia of childhood is a disease that sometimes pops up on exams and you should probably be familiar with. 05:08 Transient erythroblastopenia of childhood or TEC shows up around six months to four years of age. 05:15 I usually think of it about a year older or two-year-old. 05:18 This is a transient phenomenon, but by transient, I mean several months not just for a few minutes. 05:25 It’s a normocytic anemia because these patients are transiently incapable of making red blood cells and it’s usually preceded by a viral illness. 05:35 Often that virus is parvovirus B19, but it might be another virus as well. 05:41 In fact, parvovirus is only implicated in the minority of cases. 05:46 There is no known cure to this, but the good news is it always gets better on its own. 05:51 So typically these children will be fine, gradually become more pale, begin getting lethargy and that progression of signs and symptoms that we discussed at the beginning of this lecture and the parent will bring them in for evaluation. 06:04 You get a CBC and you notice they have a pure erythrocyte aplasia. 06:08 We will now watch these patients for a period of time, sometimes they require transfusions and then over a few months, they get better. 06:16 Flipside is when a child never develops those red cells in the first place. 06:21 They start off with red blood cells because they have fetal hemoglobin, but then they’re incapable of making any further. 06:27 This is a congenital erythrocyte aplasia. 06:31 It presents soon after birth with a rapid onset anemia. 06:36 And there is a predisposition to cancer in these patients even after they’re anemic. 06:43 One-third of cases will remit in the first decade, but many of these patients after multiple transfusions simply go on to a bone marrow transplant. 06:53 Bone marrow transplant is obviously not benign, so we want to approach this with care, but that is really the only cure for these patients who have persistent disease.
About the Lecture
The lecture Pediatric Iron Deficiency Anemia, Vitamin B12 Deficiency, Folate Deficiency & Erythrocyte Aplasia by Brian Alverson, MD is from the course Pediatric Hematology. It contains the following chapters:
- Iron Deficiency Anemia
- Vitamin B12 and Folate Deficiency
- Erythocyte Aplasia
Included Quiz Questions
Which of the following could be a dietary cause of iron deficiency anemia in young children?
- High amounts of cow's milk
- Intake of dietary sources with high bioavailability of iron
- High amounts of poultry
- High amounts of fish
Which of the following is NOT a cause of iron deficiency anemia in children?
- Thalassemia
- Celiac disease
- Inflammatory bowel disease
- Strict vegetarians
- Giardiasis
Which of the following vitamins is most likely to be deficient in a 15-year-old boy with megaloblastic anemia?
- Vitamin B12
- Vitamin C
- Vitamin B1
- Vitamin E
- Vitamin A
Which of the following characterizes Transient Erythroblastopenia of Childhood (TEC)? Select all that apply.
- It usually only lasts several months.
- It is most commonly caused by bacterial infections.
- It leads to a permanent decrease in red blood cell production.
- The anemia is normocytic.
- It is often preceded by a viral illness.
Author of lecture Pediatric Iron Deficiency Anemia, Vitamin B12 Deficiency, Folate Deficiency & Erythrocyte Aplasia

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
