Playlist
Show Playlist
Hide Playlist
Tuberculosis (TB) in Children: Management

-
Slides TB Alverson.pdf
-
Download Lecture Overview
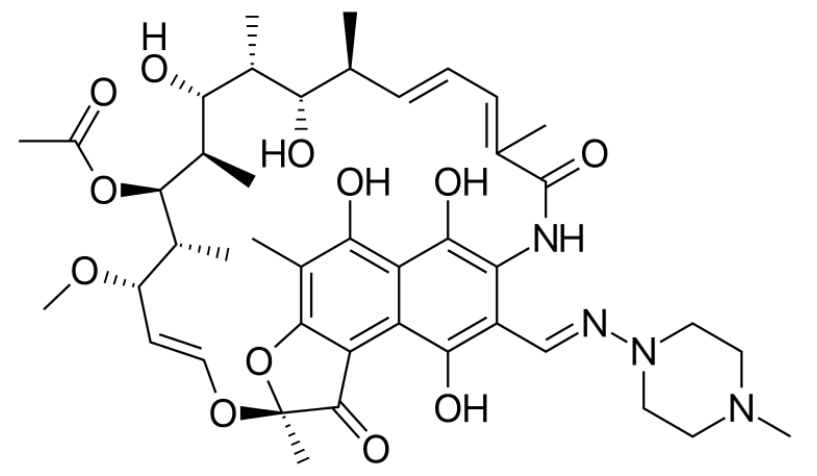
00:00 So we manage latent TB slightly differently. Typically, what we'll do for these patients is we will provide them 9 months of isoniazid or 3 months of isoniazid plus rifampin. That usually does the trick and these patients generally do not go on to develop full TB. It's about 80 to 90% effective but if we believe this patient actually has tuberculosis, we're going to use a full regimen to treat them. We'll usually tailor-regimen to both rates of resistance in the community if we are empirically treating or even better we'd like to get that culture so we know exactly what to treat it with. There is a way you can remember what are the drugs that treat tuberculosis and it's the phrase RIPES. So RIPES are the drugs that treat this particular bug. 00:56 Let's start with R. R is rifampin, I is isoniazid, P is pyrazinamide, E is ethambutol and then less commonly used or an alternative is streptomycin. Let's go through the issue about how you would choose a regimen and under what circumstances. So if you had conventional therapy for susceptible organisms, typically we're going to do for the first 2 months a multi-drug regimen of rifampin, isoniazid and pyrazinamide and then 4 months of just rifampin and isoniazid and usually that will do the trick. However, if there is a possibility of resistant organisms or your patient has HIV, we're going to do 1 of 3 regimens: RIPE, RIPS, or RIPES. That just tells you which drugs are being used. Generally, it's rifampin, isoniazid, pyrazinamide plus minus ethambutol or streptomycin depending on what's going on in your community. If the patient has isoniazid- resistant tuberculosis, we may do rifampin + ethambutol for 12 months plus minus pyrazinamide. 02:08 If it's a multi-drug resistant organism, we're going to use a combination of at least 3 drugs to which the organisms are susceptible. So, there's a lot of variability in how we care based on the context of the patient, what's going on in that community where the child received the drugs or if you can do it the culture and the culture is always key. If we're going to be using these drugs, some of them have unique side effects. It is important for us to always understand the side effects of all the drugs we use. For isoniazid, the key thing here is seizure and the reason why seizure is so key is that we treat the seizure differently than other seizures by giving vitamin B6. Remember, isoniazid-induced seizure needs to be treated with an extra dose of vitamin B6. 03:02 Roughly 10% of these patients will develop a hepatitis and it can be rarely severe. The way you might remember the side effects of isoniazid is INH. Isoniazid causes neurologic and hepatitis. 03:17 Okay, rifampin. Rifampin causes GI upset, hepatitis, rash, thrombocytopenia and cholestasis. 03:27 The thing to remember about rifampin though is you look like an orange Gatorade commercial. 03:32 You remember those commercials where they have orange coming out of their eyes and their sweat? These patients will have orange everything. Their pee will be orange, their sweat will be orange, it will get on their clothes, their tears will be orange. You should definitely warn them about the side effect. For pyrazinamide, the drug is usually well tolerated in children and the side effects are less unique: GI upset, rash, hepatitis. For ethambutol, the key one to remember is retrobulbar neuritis, blurry vision and sometimes a red/green color blindness. So, how do we prevent TB in the first place? You're probably confused or maybe you're not but I was certainly confused as a student about why the BCG vaccine is used in some places and not on others. 04:25 The BCG vaccine is only effective at reducing severe disease but it doesn't prevent you from getting the disease. What this means is it's useful in countries where there is a high prevalence. 04:38 Generally, these are developing nations. It's not so useful in areas where there's a low prevalence because it prevents you from getting severe disease but doesn't prevent you from actually getting the disease. The other reason why it's challenging is because in countries where this disease isn't very prevalent, we can effectively use the PPD as a screen. If you imagine, if we were to go to a country where TB is rampant throughout, doing a PPD everywhere and checking and then treating for a short period of just isoniazid therapy or isoniazid + rifampin therapy for an exposure would be very ineffective, everyone's got a positive PPD. So, the BCG, it doesn't matter that it prevents PPD screening because they are not going to do that in that country. They're going to be trying to reduce people from getting severe disease. In developed countries where this is less common, the PPD screen is an effective way of screening through the population and we do it in lots of children. So, we usually use PPDs rather than BCGs in developed countries like the United States. In countries with low prevalence, screening with PPD alone is more effective. 05:56 Another big part of prevention is making sure that people who have the disease are isolated. 06:02 In the hospital, we're going to use N-95 masks and we're going to use negative pressure rooms so they can't spread their disease throughout. Also, it's actually legal to force patients who are reluctant to take their TB medicine. This is a public health problem. So there may be government sanctioned or judge sanctioned observed therapy we called direct observed therapy in patients with this disease. So that's my summary of Tuberculosis in Children. Thanks for your time.
About the Lecture
The lecture Tuberculosis (TB) in Children: Management by Brian Alverson, MD is from the course Pediatric Infectious Diseases.
Included Quiz Questions
Which of the following is NOT a medication used to treat tuberculosis?
- Erythromycin
- Rifampin
- Isoniazid
- Pyrazinamide
- Streptomycin
Which of the following is an appropriate treatment regimen for an HIV-positive patient with tuberculosis?
- Rifampin, isoniazid, pyrazinamide ± ethambutol or streptomycin
- Rifampin, isoniazid ± pyrazinamide
- Rifampin, isoniazid, and ethambutol
- Rifampin, pyrazinamide ± streptomycin
- Rifampin and isoniazid
How many months of isoniazid is given to a patient with latent tuberculosis?
- 9 months
- 6 months
- 3 months
- 12 months
Which of the following drugs may cause orange-colored urine as a side effect?
- Rifampin
- Isoniazid
- Pyrazinamide
- Ethambutol
- Streptomycin
What is the treatment for a seizure caused by the drug isoniazid?
- Vitamin B6
- Vitamin B1
- Vitamin B12
- Vitamin C
- Folic acid
What type of color blindness may be a side effect of ethambutol use ?
- Red / Green
- Red / Blue
- Red / Yellow
- Green /Blue
- Green / Yellow
Author of lecture Tuberculosis (TB) in Children: Management

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Good explanation of drug side effects and easy to remember
I particularly liked the explanation regarding PPD and prevalence in poor/rich countries.
