Playlist
Show Playlist
Hide Playlist
Actions of ADH

-
Slides ActionOfADH EndocrinePathology.pdf
-
Download Lecture Overview
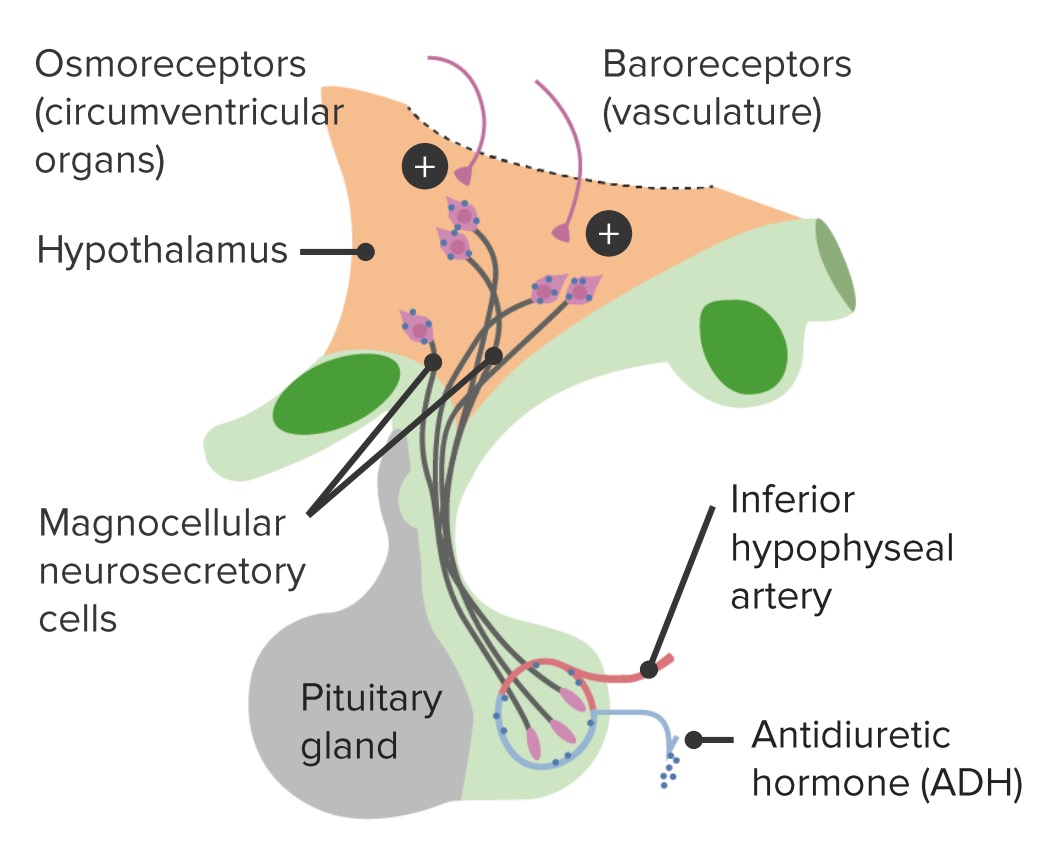
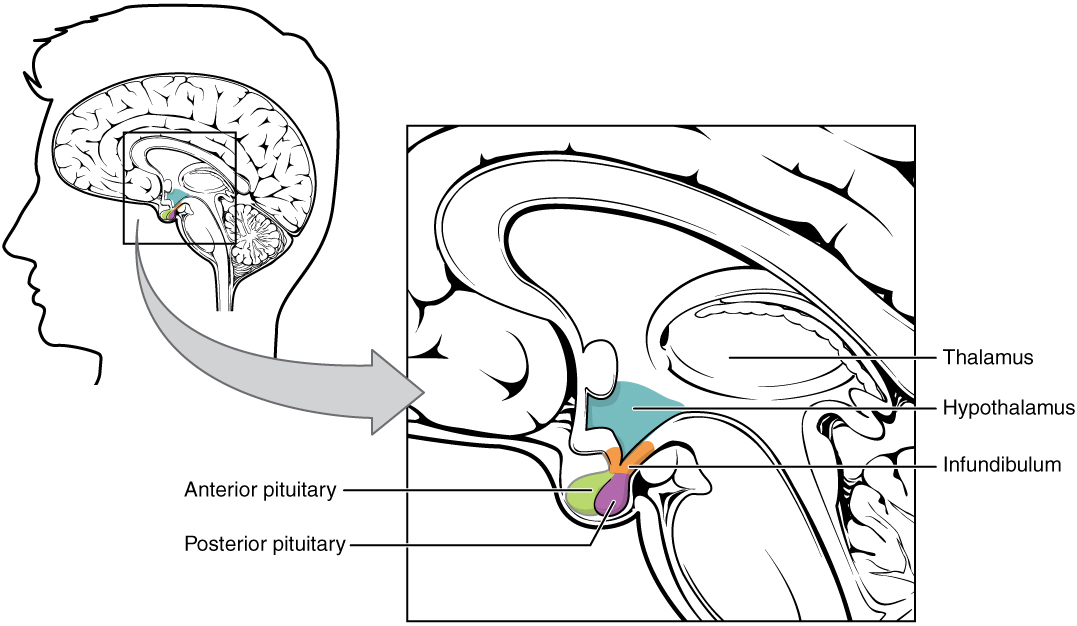
00:01 Let’s take a look at the Posterior Pituitary. 00:06 At first, real posterior pituitary hormone here is ADH. 00:11 Now, even though there are only two hormones that we will be addressing here with posterior pituitary, my goodness, the clinical applications of these are massive, as you shall see. 00:22 First, what is this particular illustration showing us? Understand where you are. 00:29 We’re in the collecting duct, we’re in the kidney and we’re moving from our cortex into the medulla and I want you to imagine that beyond the collecting duct versus urine osmolality of being 1200, beyond this, we’re going into our minor/major calyces and then out towards the pelvis and towards the-towards the ureter. 00:53 Are we clear as to where we are now? This is not the loop of Henle; we are in the kidney and we are in the level of the collecting duct and then here, with ADH, we’ll be referring to its receptor being V2 receptors. 01:07 And with V2 receptors, remember we talked about the vasopressin with V2 receptors and its second messenger here will be Gs in fact… not Gq, but Gs. 01:18 So, in the distal convoluted tubule that’s responsible for increased water reabsorption, thus with the help of ADH only in the collecting duct can it move up to 1200. 01:30 Now, they can ask you a physio question here by saying that without the effective ADH on the nephron, where is it in the nephron that your urine osmolality will be the highest? It would have to be the loop, right? Are you picturing? And by that, I mean the descending loop of Henle where you are reabsorbing your water, but that has nothing to do with ADH, does it? Right? It’s only after you’ve understood that point in which this sentence here where, with the help of ADH and V2 receptors reabsorbing water, you then form concentrated urine. 02:08 Next, a different location all together. 02:13 This is not-not the collecting duct, this is not the nephron. 02:20 This is in reference to ADH and its effect via V1 receptors on your blood vessels where we are here. 02:28 Look at the arrows that you see here with ADH and with the help of it, you’ll notice that the blood vessel here on top is a lot more narrow in calibre than it is at the bottom. 02:40 It kind of looks like a flask. 02:42 And the only reason that it looks like this is because when a patient is dehydrated, when releasing ADH, it is responsible for vasoconstriction and this will be V1. 02:58 Along with this, understand that ADH will then promote the release of von Willebrand factor and factor VIII via endothelium. 03:08 Endothelium, of course, being the cells of your blood vessel and you should remember that von Willebrand factor and factor VIII work together for optimum, optimum haemodynamic functioning. 03:23 So, vasopressin analogues for the management of von Willebrand type 1 and hemophilia could be used effectively, can’t it? Amazing management vignette here, isn’t it? It’s a fact that you may use an analogue of vasopressin. 03:45 If you’re thinking about von Willebrand disease type 1, understand that you’re deficient of von Willebrand factor. 03:51 And if you’re deficient of van Willebrand factor, you remember that patient who has massive menorrhagia and the fact that you have increase in bleeding time in PTT, why? Because you need von-von Willebrand factor for optimum functioning of factor VIII. 04:08 So, therefore, a vasopressin analogue could in fact be used in this condition. 04:15 And then what about haemophilia A? Haemophilia A is strictly deficiency of factor VIII. 04:21 Hence, you would only find an increase in PTT. 04:24 Here, once again, vasopressin could be used to perhaps manage your patient with haemophilia A by releasing factor VIII. 04:38 At supra-physiologic levels of ADH, it works on V1 receptors to cause vasoconstriction. 04:44 It is important for you to understand that. 04:46 So, you need really high levels of ADH, so you need to have a patient who is quite severely dehydrated in which the influence of ADH on your blood vessels would be taking place. 05:01 At low levels of ADH, as soon as our plasma osmolality rises, let’s say above 300, then your ADH will be released from the posterior pituitary. 05:13 Just to keep things into perspective, ADH is being synthesized where? In the hypothalamus.
About the Lecture
The lecture Actions of ADH by Carlo Raj, MD is from the course Pituitary Gland Disorders.
Included Quiz Questions
A patient with heart failure presents with edema, hyponatremia, and concentrated urine. Activity of which receptor is most likely to be contributing to these symptoms?
- Vasopressin receptor 2 in the collecting duct of the kidney
- Vasopressin receptor 2 in the descending loop of Henle
- Vasopressin receptor 1 in the cortical collecting tubule
- Vasopressin receptor 1 in the vascular endothelium
- Vasopressin receptor 2 in the vasa recta
Why is a vasopressin analog effective in the treatment of hemophilia A?
- It stimulates the release of von Willebrand factor and increases factor VIII levels.
- It inhibits the release of von Willebrand factor by increasing factor VIII levels.
- It increases factor VIII levels without affecting von Willebrand factor.
- It stimulates the release of von Willebrand factor without affecting factor VIII levels.
- It inhibits the release of von Willebrand factor by decreasing factor VIII levels.
What is NOT an effect of vasopressin or its synthetic analog?
- Urine dilution
- Vasoconstriction
- Stimulation of clotting
- Intravascular volume repletion
- Plasma osmolarity regulation
Which condition is most likely to activate vasopressin receptor 1 via very high levels of vasopressin?
- Hypovolemic shock
- Severe hyperosmolarity
- Bleeding in hemophilia A
- Severe edema
- Sheehan syndrome
Author of lecture Actions of ADH

Carlo Raj, MD
Customer reviews
3,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
1 |
This guy is definition of PERFECTION. The way he explains, makes me laugh all the time. Thanks Carlo Raj.
It is hard for me to listen to his speech, He is stressing every word and I feel the teacher being arrogant
