Playlist
Show Playlist
Hide Playlist
NSAIDs Induced Peptic Ulcer Disease

-
Slides Stomach and Duodenum.pdf
-
Download Lecture Overview
00:00
NSAID Associated Peptic Ulcer Disease. Your patient
taking, let’s say NSAIDs for osteoarthritis
or in general, just inflammation of the
joints. Have been taking this over decades.
00:17
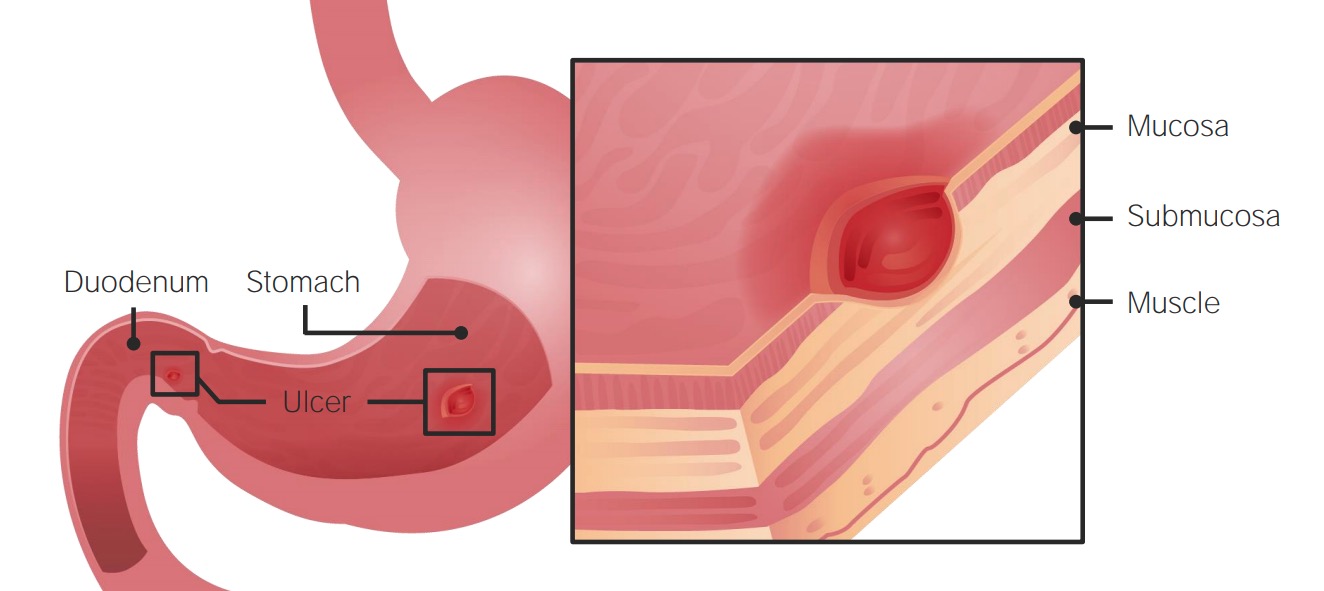
And with NSAIDs as we mentioned earlier, if the
prostaglandins are then lost within the stomach,
the lining of the stomach in fact now becomes vulnerable
to the acid abuse and so therefore may bring about
erosion of the lining resulting in peptic ulcer disease
of the stomach. The first case that you’re going to
find with peptic ulcer disease of the stomach but
long term use, you consider this to be acute.
00:43
And it’s not like you take one aspirin or you take
one ibuprofen and then all of a sudden the patient
develops peptic ulcer disease. That makes no sense.
You have to be taking these drugs over a long period
of time. Also keep in mind, though, if NSAIDs
are being taken over long period of time
that in the kidney, with prostaglandins responsible
for keeping the afferent arteriole open.
01:10
If NSAIDs are taken, you take out the prostaglandin,
you’re at risk of vasoconstricting the afferent
and over a long period of time, here as well,
you’re worried about chronic kidney injury.
01:23
Is that clear? Two major organ systems that are
extremely vulnerable to attack with NSAID use.
01:30
And really because of the easy accessibility of these
drugs by the patient over the counter, you have to
properly educate your patient because they’re going
to be popping pills all of the time whenever they
feel pain. And I’m talking popping pills excessively
for long period of time. And they may or may not
even tell you. Right? Increased risk of
bleeding with low dose and high dose aspirin.
01:55
Further increased risk of dose dependencies which
you’re worried about. Exactly what I was saying,
the patients are in pain, they might be taking aspirin
and they might be increasing the dosage without
you ever knowing. It is important that you establish
in your practice, excellent rapport with your patients.
02:15
So that they're being transparent between you and
your patient. Enteric coating does not reduce
the risk of bleeding. Do not allow the advertisements
and the commercials to fool you. High rate of
mortality for NSAID associated with GI bleeding.
02:35
Who is your patient with NSAID associated peptic
ulcer disease. More than 70, higher dose of NSAIDs,
often associated with H. pylori, and concomitant
corticosteroids. Remember please, with NSAIDs,
they might very well be in pain and if they are,
they’re probably taking prednisone as well.
02:58
My goodness. A combination of NSAIDs and corticosteroids
definitely compromises the production of
your prostaglandin. Therefore increases the risk of
peptic ulcer disease further. Also, anticoagulants.
03:13
Prior history of peptic ulcer disease.
03:16
NSAIDs what does it do? Inhibits your prostaglandin.
Management. PPI and remove the NSAIDs.
03:24
At some point in time if peptic ulcer disease
has kicked in, remove the offending agent.
03:30
Educate your patient properly and PPIs. Always treat
your H. pylori. Highly indicated gastric or duodenum.
03:39
H. pylori, for the most part, you assume is present.
03:45
Prophylaxis. Misoprostol, a prostaglandin. It’s a
prostaglandin E derivative and combats the effects
of NSAIDs. Diarrhea is a dose limiting side effect
however. And absolutely contraindicated in pregnancy.
04:06
Prophylaxis. PPI. Superior to H2 blockers we’ve
talked about when it comes to acid control.
04:14
COX−2 inhibitors might be a possible alternative.
Lacks cardiovascular protective effect.
04:22
And GI protective effect lost with concomitant baby
aspirin use. So COX−2 inhibitors, you've heard of
celecoxib, so on and so forth. Might be alternatives
that you’re looking for when dealing with NSAID
associated peptic ulcer disease.
About the Lecture
The lecture NSAIDs Induced Peptic Ulcer Disease by Carlo Raj, MD is from the course Stomach and Duodenum Diseases: Basic Principles with Carlo Raj.
Included Quiz Questions
What is the percentage of risk of a GI bleed seen in patients using long-term NSAIDs?
- 1.3%
- 1.6%
- 1.7%
- 1.9%
- 2.3%
How do NSAIDS that are used adversely affect the kidneys?
- By vasoconstriction
- By increased capillary permeability
- By vasodilation
- By lowering blood pressure
- By thinning of the blood
Which drug used in conjunction with NSAIDs can lead to an increase in NSAID-related peptic ulcers?
- Prednisone
- Thyroxine
- Codeine
- Morphine
- Lidocaine
Author of lecture NSAIDs Induced Peptic Ulcer Disease

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
such a good lecuture. Covers the topic in a broad sense. good clinical value.
