Playlist
Show Playlist
Hide Playlist
Aortic Stenosis: Signs and Symptoms

-
Slides ValvularHeart DiseaseAorticStenosis CardiovascularPathology.pdf
-
Download Lecture Overview
00:01
The triad that you are looking for chest pain
sure with that bigger thickness of the left
ventricle wall you are going to have angina
because it may perhaps you can't supply enough
blood. Heart failure, late finding, remember
early on, the left ventricle is lifting weights.
00:16
And so therefore, is it possible that your
ejection fraction could be preserved early
on in aortic stenosis? Sure it can. So your
ejection fraction would be what exactly? Your
stroke volume over EDV, isn't it? So therefore
when you have aortic stenosis early on, your
ejection fraction could actually be preserved.
Please be careful. Do not confuse that with
congestive heart failure as we shall see later
on. Now as you continue and there isn’t
proper management of your patient's aortic
stenosis, guess what happens? The ejection
fraction is going to get compromised and you
will go into major heart failure. And if you
do, at that point, that is a bad prognostic
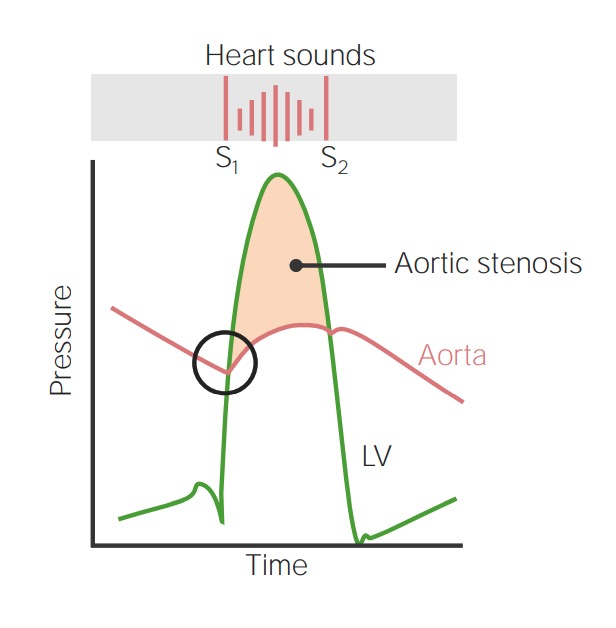
indicator. Here we go. Here is your S1 and S2.
01:00
What did we say about this? A crescendo
descrescendo because the aortic valve doesn't
want to open immediately. Tell me about the
left ventricular pressure. Increased or decreased
in comparison to aortic pressure? Increased
left ventricular pressure. You remember the area
underneath that curve. The discrepancy between
those two curves represents aortic stenosis.
01:19
Where do you hear this? Right upper area.
You will find that in right upper second intercostal
space. That is where you will find aortic
stenosis to be the loudest. It will be radiating
where? To the carotid. And last in terms of
S2 well, which second heart sound will then
close first? Pulmonic followed by aortic,
which is called paradoxical splitting. Remember
that. So with S2, I told you that there are
particular heart sounds that you want to pay
attention to physiologic versus widened versus
fixed and in this case we have paradoxical.
02:03
The physical examination, you would expect
the left ventricle to work really hard because
of increased pressure. And so therefore it will
be hyperdynamic and it is enlarged, but it
is left ventricular hypertrophy. You want
to make sure that you catch your patient early
on with aortic stenosis because if that ejection
fraction starts dropping, what I say about
prognosis? Dismal. You don’t want that happen.
So I need you to be astute please. Next, an important
point is this. Something called pulsus parvus
et tardus. What this mean is slow and late
carotid pulse due to what? Pay attention here.
Left ventricle wants to eject blood during
when? During systole. Your patient has bicuspid
aortic valve. Well what kind of calcification?
Dystrophic. Resulting in? Aortic stenosis. What
happened to cardiac output? Decreased. So
when you have decreased cardiac output, then
what happens to the pulse and such? It is
delayed. So slow and late is what is called
pulsus parvus et tardus. Slow and late carotid
pulse due to what? Delay in blood flow across
that stenotic aortic valve. It is that simple
for you to understand. Are you going to
have differential pressures here? No such
thing. Differential pressure gives me diagnosis.
"What do you mean differential pressure, Dr. Raj?"
Increased pressure in upper extremity,
lower pressure in the lower extremity, that
is differential pressure. What is your diagnosis?
That you are coarctation of the aorta. So
be careful when you try to bring in differentials here.
About the Lecture
The lecture Aortic Stenosis: Signs and Symptoms by Carlo Raj, MD is from the course Valvular Heart Disease: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following features is not associated with aortic stenosis?
- Holosystolic murmur
- Paradoxical splitting of S2
- Pulsus parvus et tardus
- Hyperdynamic and enlarged left ventricle
- Syncope
What characterization of the heart sounds is heard with aortic stenosis?
- S2 with the pulmonic valve closing prior to the delayed closure of the aortic valve.
- A widely split S1 sound
- A widely split S2 sound
- Physiologic splitting of the second heart sound with the aortic valve closing first and the pulmonic closing second
- No splitting of the second heart sound as the aortic and pulmonic valves close at the same time.
Author of lecture Aortic Stenosis: Signs and Symptoms

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Amazing explanations each lecture! Thank you so much, Dr. Raj!
