Playlist
Show Playlist
Hide Playlist
Insulinoma (Whipple's Triad) with Case

-
Slides 02-03 Diabetes Mellitus part 2.pdf
-
Download Lecture Overview
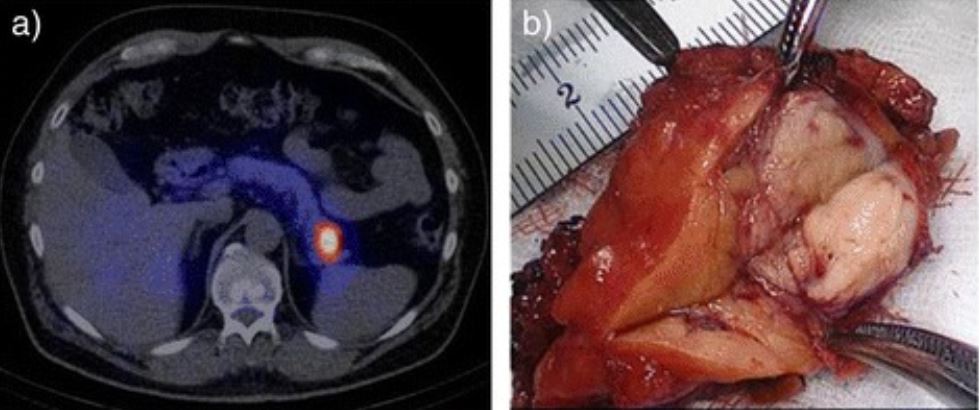
00:00 Let's go on to another case. A 25-year-old female presents to the emergency department with palpitations, sweating, and blurry vision after playing volleyball on the beach. She denies chest pain and shortness of breath. She states that these symptoms occur often, but resolved after eating a meal or drinking a sugary soda. Past medical history is unremarkable and she takes no medications. 00:26 Temperature is 37°C, blood pressure 135/80, pulse rate 102 beats/minute, and respirations 18. Fingerstick blood glucose level is 42 mg/dL. ECG revealed sinus tachycardia. Urine analysis and toxicology are non-contributory. Appropriate medical therapy is administered and she is discharged with an appointment for a fasting blood draw within the week. These labs show a blood glucose of 14 mg/dL, a C-peptide of 0.8 nmol/L, a serum insulin of 20 microU/L, a serum pro-insulin of 10 microU/L, a negative sulfonylurea, and a negative IGF2. The symptoms of palpitation, sweating, blurred vision all resolved with food and implied the presence of underlying hypoglycemia. This is confirmed on a fingerstick blood glucose and then repeated by a serum blood glucose in both cases revealing low blood glucose or hypoglycemia. The patient's C-peptide level is 0.8 nmol/L. This implies that there is some degree of endogenous insulin production and this is again confirmed by an elevated level of serum insulin and pro-insulin. The sulfonylurea is negative which suggests that she is not taking an oral hypoglycemic. The most likely diagnosis here in this young girl is an insulinoma. Normally, pro-insulin is cleaved into insulin and C-peptide and both are secreted from the pancreas into the bloodstream. Endogenous insulin is manufactured in its active state. It is not cleaved and will not change the C-peptide levels. To rule out insulin overdose or factitious disorder, pro-insulin and C-peptide levels are measured. The patient's C-peptide levels are elevated indicating that she did not inject insulin surreptitiously. Further work-up must be completed for this patient including imaging, ultrasound, CT scan, or MRI of the abdomen to assess for a pancreatic insulinoma. Evaluation for pathologic hypoglycemia. 02:47 When Whipple's triad is present namely symptomatic hypoglycemia, hypoglycemia at less than 55 mg/dL, and the prompt symptomatic relief with the correction of the hypoglycemia. No confirmation of hypoglycemia with glucose monitors but instead use the more accurate serum laboratory method to confirm the fingerstick. The etiology of hypoglycemia in patients without diabetes is mostly caused by drugs. Illness, however, hormone deficiencies, non-islet cell tumors, endogenous hyperinsulinism or non-insulinomas, and pancreatogenous hypoglycemia may be rarer causes. Depletion of hepatic glycogen stores may also contribute. Alcohol ingestion and finally intentional or unintentional use of hypoglycemic agents is also a common cause.
About the Lecture
The lecture Insulinoma (Whipple's Triad) with Case by Michael Lazarus, MD is from the course Diabetes Mellitus. It contains the following chapters:
- Case: 25-year-old Woman with Palpitations and Sweating
- Symptomatic Hypoglycemia
Included Quiz Questions
What is most likely the appropriate medical therapy applied in the case described below? A 25-year-old woman presents to the emergency department with palpitations, sweating, and blurry vision after playing volleyball on the beach. She denies chest pain and shortness of breath. She states that these episodes occur often but resolve after eating a meal or drinking a sugary soda. Past medical history is unremarkable, and she takes no medications. Physical examination: Temperature is 37.0°C (98.6°F), blood pressure is 135/80 mm Hg, pulse is 102 beats/min, and respiration rate is 18 breaths/min. Laboratory test results: Fingerstick blood glucose level is 42 mg/dL, electrocardiography shows sinus tachycardia, and urinalysis and toxicology results are noncontributory. Appropriate medical therapy is administered, and she is discharged with an appointment for a fasting blood draw within the week. Laboratory test results: Blood glucose is 45 mg/dL, serum proinsulin is 10 µU/L, C-peptide level is 0.8 nmol/L, results for sulfonylurea are negative, serum insulin level is 20 µU/L, and results for IGF-2 are negative.
- 15–20 g of glucose
- Intravenous insulin
- Subcutaneous insulin
- Beta-blocker
- 0.9% saline with 10% dextrose at 1 L/hour
Which of the following constellations of laboratory findings is most suggestive of factitious insulin injection when found in a hypoglycemic patient?
- High serum insulin and low C-peptide levels
- High serum insulin and high C-peptide levels
- High serum insulin level and positive GAD antibodies
- Low blood glucose, low serum insulin, and elevated serum sulfonylurea levels
- High serum proinsulin level and negative serum sulfonylurea
What is the most likely diagnosis in the following case? A 25-year-old woman presents to the emergency department with palpitations, sweating, and blurry vision after playing volleyball on the beach. She denies chest pain and shortness of breath. She states that these episodes occur often but resolve after eating a meal or drinking a sugary soda. Past medical history is unremarkable, and she takes no medications. Physical examination: Temperature is 37.0°C (98.6°F), blood pressure is 135/80 mm Hg, pulse is 102 beats/min, and respiration rate is 18 breaths/min. Laboratory test results: Fingerstick blood glucose level is 42 mg/dL, electrocardiography shows sinus tachycardia, and urinalysis and toxicology results are noncontributory. Appropriate medical therapy is administered, and she is discharged with an appointment for a fasting blood draw within the week. Laboratory test results: Blood glucose is 45 mg/dL, serum proinsulin is 10 µU/L, C-peptide level is 0.8 nmol/L, results for sulfonylurea are negative, serum insulin level is 20 µU/L, and results for IGF-2 are negative.
- Insulinoma
- Excessively high dose of an oral hypoglycemic drug
- Type 1 diabetes mellitus
- Glycogen storage disorder
Author of lecture Insulinoma (Whipple's Triad) with Case

Michael Lazarus, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Case studies helped with a better understanding and linking underpinning theory to clinical practice. Touched on all key aspects of the challenges of diabetes and its short and long term complications.
