Playlist
Show Playlist
Hide Playlist
Hypothalamic and Pituitary Hormone Deficiency

-
Slides 01-02-01 Adrenal Pituitary.pdf
-
Download Lecture Overview
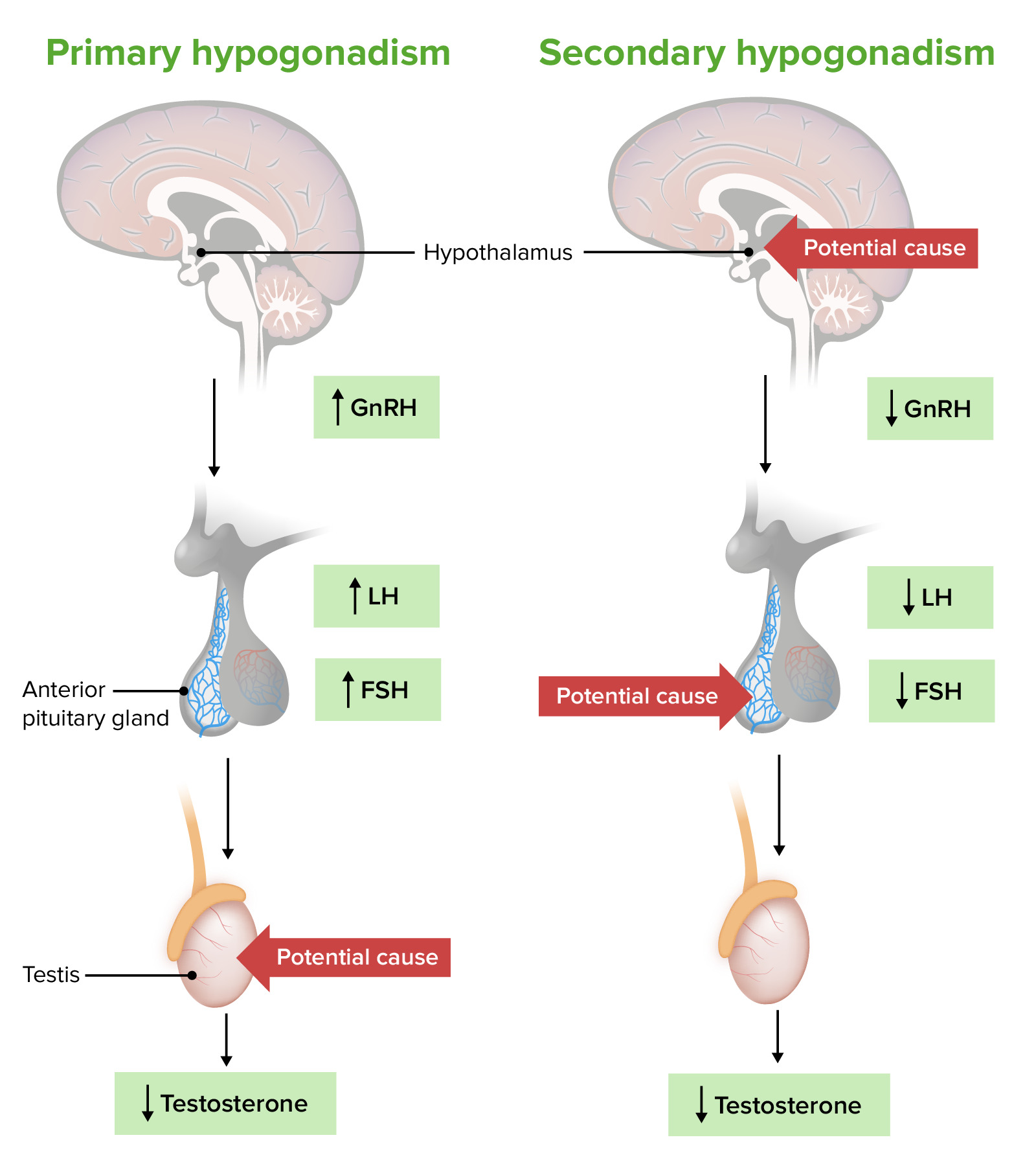
00:00 Let's talk about hypothalamic and pituitary hormone deficiency. In the anterior pituitary gland, deficiencies of ACTH manifest a secondary cortisol deficiency. Thyroid stimulating hormone manifests central hypothyroidism and this is covered in the thyroid section. Gonadotropin deficiency can manifest with amenorrhea. Growth hormone deficiency in individual's prepuberty manifests with prolactin hormone deficiency. In the posterior pituitary gland, oxytocin may be decreased and antidiuretic hormone may be decreased resulting in central diabetes insipidus versus peripheral diabetes insipidus. There are a number of pituitary hormone deficiency states; hypopituitarism, pituitary apoplexy, and growth hormone deficiency. The causes of hypopituitarism include pituitary adenomas, pituitary surgery, pituitary radiation, apoplexy or infarction. Craniopharyngiomas, metastatic tumors, even meningiomas can cause compression of the pituitary. Lymphocytic hypophysitis and sarcoidosis are much rarer manifestations as of the conditions listed here. One or more pituitary hormone deficiencies is usually the definition of hypopituitarism. Growth hormone, FSH, LH are the most sensitive hormones to injury and the most commonly deficient. Panhypopituitarism, on the other hand, is the situation where the patient lacks all of the anterior pituitary hormones. This is usually due to a very large tumor or pituitary surgery. There is a need to replace thyroxin and cortisol in the setting. 01:52 Replacement of 6 steroids and growth hormone depend on the age of the patient and the clinical benefits. Secondary cortisol deficiency is commonly iatrogenic due to exogenous glucocorticoid suppression of pituitary ACTH secretion. Patients with secondary cortisol deficiency have only glucocorticoid deficiency and the rest of the adrenal gland functions normally as does the renin angiotensin system. They're at less risk for hypotension and hyponatremia and adrenal crisis than those with primary cortisol deficiency because the production of mineralocorticoid is retained. Unlike patients with primary cortisol deficiency, patients with secondary cortisol deficiency do not develop hyperpigmentation or bronzing of the skin. This is because ACTH and its prohormone which is responsible for these changes, proopiomelanocortin or POMC is not hypersecreted. TSH deficiency leads to secondary or central hypothyroidism. 02:58 Secondary hypothyroidism is clinically identical to primary hypothyroidism. Thyroid-stimulating hormone deficiency can be diagnosed by demonstrating a simultaneously inappropriately normal or low TSH level with a low T4 either free or total. The treatment involves levothyroxine replacement for primary hypothyroidism. Serum TSH cannot be used to monitor and assess for adequacy of thyroid hormone replacement. Levothyroxine dose is adjusted based on free T4 levels with a goal of obtaining a value within the normal reference range. Growth hormone deficiency prior to puberty will lead to short stature. In adulthood, growth hormone production is not as important for growth as during childhood. In adults, growth hormone deficiency causes fatigue, loss of muscle mass, and increase in the ratio of fatty tissue to lean tissue and increased risk for osteoporosis. Evaluation for growth hormone deficiency is recommended in patients with at least 1 known pituitary hormone deficiency. Unfortunately, growth hormone therapy has been used inappropriately as an alternative medication without good evidence to support its use. Let's talk about gonadotropin-releasing hormone deficiency. 04:21 The pituitary gland normally secretes LH and FSH in response to GNRH from the hypothalamus. 04:28 Luteinizing hormone and follicle stimulating hormone stimulates the secretion of normal male and female sex hormones. LH and FSH deficiency causes hypogonadotropic hypogonadism. 04:43 Causes include hypothalamic amenorrhea in women associated with excess exercise as seen in professional athletes or severe illness or anorexia. Congenital GnRH deficiency is seen in Kallmann syndrome. This condition occurs when hypothalamic neurons responsible for releasing GnRH fail to migrate into the hypothalamus during embryonic development. The treatment, if fertility is the goal, replace gonadotropins in men and women. In women who are premenopausal who do not desire fertility, estrogen and progesterone containing oral contraceptives should be provided. Treatment also is recommended to avoid loss of estrogen dependent bone at a young age which could lead to osteoporosis. Postmenopausally, hypogonadotropic hypogonadism treatment is not indicated. In men, if fertility is not desired testosterone replacement therapy can be offered.
About the Lecture
The lecture Hypothalamic and Pituitary Hormone Deficiency by Michael Lazarus, MD is from the course Pituitary and Hypothalamic Disorders. It contains the following chapters:
- Hypothalamic and Pituitary Hormone Deficiency
- Pituitary Hormone Deficiency States
- Adrenocorticotropic Hormone Deficiency
- TSH Deficiency
- GH Deficiency
- Gonadotropin (GnRH) Deficiency
Included Quiz Questions
Which of the following diseases is caused by a deficiency of antidiuretic hormone (ADH)?
- Diabetes insipidus
- Diabetes mellitus
- Cushing disease
- Addison disease
- Cushing syndrome
Which hormone deficiencies are more frequent during early anterior pituitary failure?
- Growth hormone, LH, and FSH
- Growth hormone, TSH, and ACTH
- TSH, ACTH, and LH
- ACTH, LH, and FSH
- Growth hormone, ACTH, and FSH
Which clinical feature suggests primary cortisol deficiency rather than secondary cortisol deficiency?
- Hyperpigmentation of skin
- Moon facies
- Malar rash
- Palmar erythema
- Livid striae
Author of lecture Hypothalamic and Pituitary Hormone Deficiency

Michael Lazarus, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
