Playlist
Show Playlist
Hide Playlist
Pediatric Diarrhea: Lab Work & Imaging

-
Slides Gastroenteritis.pdf
-
Download Lecture Overview
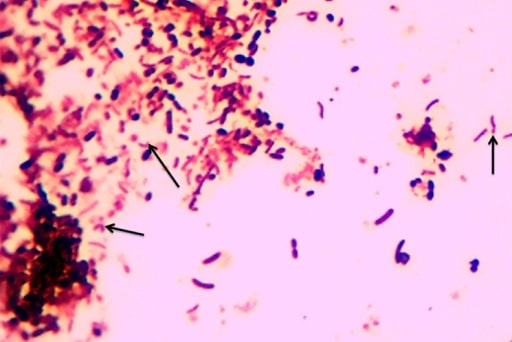
00:02 So what lab work would you get? Again, serum electrolytes. 00:06 You might get stool bacterial cultures. 00:09 The question is if this is cost effective, because the reality is the vast majority of bacterial enteritis, we do not treat with antibiotics. 00:19 They get better on their own. 00:21 In fact, there was some evidence that the varieties of E. coli that cause hemolytic uremic syndrome may be more likely to cause hemolytic uremic syndrome if treated. 00:32 We really reserve treatment of bacterial enteritis for Shigella, Salmonella that’s severely bad or in children under three months of age, or a child who simply isn’t getting better from the bacterial enteritis. 00:48 There is now emerging stool PCR panels that are very effective at picking up a variety of illnesses that can cause gastroenteritis. 00:59 These panels are available through rectal swab or through stool collected and sent to the lab. 01:08 Right now, the cost for these panels is very high. 01:11 At our hospital, it costs upwards of $800. 01:14 So it’s important to have a very good reason why you’re getting this test. 01:17 If it’s preventing a child from going to the operating room for endoscopy, it’s probably worth it. 01:23 But if it’s just to see what it is, it might not be. 01:27 Waiting for the child to get better may be your best option. 01:31 Stool microscopy for ova and parasites may be effective in a child who you suspect has an ova and parasite, however, remember this is also costly. 01:42 It’s labor-intensive in the lab. 01:45 And so don’t send it on every patient. 01:47 Really limit it to patients where you strongly suspected a parasite. 01:50 For example, someone who’s recently been abroad. 01:54 If you’re suspecting hemolytic uremic syndrome and we will talk about that more in another lecture, it’s critically important to assess renal function to test for E. coli O15:H7. 02:06 And of course, to get a CBC to look for thrombocytopenia and anemia. 02:12 If you suspect failure to thrive in a child, the child is not gaining weight and this is associated with prolonged diarrhea. 02:21 It’s important to consider cystic fibrosis. 02:25 Tests we can get include stool elastase, but the cheapest test and the easiest test is simply is a sweat test. 02:32 For inflammatory bowel disease patients, we might check for elevated inflammatory markers such as the ESR, the sed rate, or the CRP. 02:41 But remember that those tests maybe normal even during an inflammatory bowel disease flare. 02:48 Probably the best test we can get is the fecal calprotectin. 02:54 For patients where we suspect malabsorption, a child with for example edema, who might have a low protein level causing them to be edematous, it can be done that we can check for things like stool-reducing substances, which would check for sugar, fecal fat, or alpha-1 anti trypsin in the stool. 03:15 If we suspect immunodeficiency, of course, getting an HIV test should be every one’s priority as well as checking for lymphocyte counts and looking at their immunoglobulin profile. 03:29 So if we have a patient has prolonged diarrhea and emesis and we, despite all those labs, cannot figure out what’s going on, we will usually proceed to endoscopy or colonoscopy, depending on which side has the problem. 03:45 So examples of this would be a child where we suspect inflammatory bowel disease. 03:50 These children, really endoscopy is the best way to make that diagnosis. 03:55 If there’s an unclear cause of malabsorption, we’ll do endoscopy to try and figure out what’s going on. 04:00 Sometimes, the biopsies can show us a problem with the brush border in the colon for example, which may give us a clue as to what’s going on and why that child is not able to absorb nutrients. 04:12 In patients with celiac disease, we think about getting the tTG and the IgA levels from the blood. 04:20 And that is how we can make a presumptive diagnosis. 04:23 But most physicians will want an actual biopsy of the intestinal wall to verify that that’s diagnosis because the diagnosis of celiac disease is a tough one to give to a patient. 04:35 Remember, they have to change their diet for the rest of their lives. 04:40 Obviously, in any patient with a severe GI bleed, we want to go do endoscopy to try and stop the bleed. 04:47 Remember GI bleeds can happen very quickly and can be very severe and life-threatening. 04:53 Lastly, certainly if we suspect suspicion for enteric disease such eosinophilic esophagitis or eosinophilic gastritis, a biopsy is necessary to truly make that diagnosis. 05:07 Also, visualization of the enteric wall may give us clues as to what’s going on. 05:13 So that’s my summary of everything that has to do with children who are vomiting or have diarrhea. 05:19 And it’s a good overview for you to keep in mind as we delve into more of these diseases in further lectures. 05:25 Thanks for your time.
About the Lecture
The lecture Pediatric Diarrhea: Lab Work & Imaging by Brian Alverson, MD is from the course Pediatric Gastroenterology.
Included Quiz Questions
Which test is a good test for inflammatory bowel disease?
- Fecal calprotectin
- Stool elastase
- Sweat test
- Lymphocyte enumeration
- IgA level
A 6-year-old girl is brought to the pediatrician with complaints of chronic diarrhea and failure to thrive. Which of the following is the LEAST likely cause?
- Amebic dysentery
- Cystic fibrosis
- Inflammatory bowel disease
- Malabsorption syndrome
- Immunodeficiency disorder
Which of the following will increase the risk of hemolytic uremic syndrome in a patient with E.coli caused diarrhea?
- Antibiotic treatment
- Malnutrition
- Dehydration
- Low body weight
- Supportive therapy
Author of lecture Pediatric Diarrhea: Lab Work & Imaging

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent lecture. Good overview of vomiting and diarrhoea with the definitions, etiologies and the most frequent diagnoses. Good explanation of the questions to ask to the parents.
Explained the topic very effectively. Made easy to understand. Also the progress of the lesson is very catchy.
