Playlist
Show Playlist
Hide Playlist
Metabolic Neuropathies and Diabetic Neuropathy

-
Slides 07 PolyneuropathyIndusIntellect Neuropathology.pdf
-
Download Lecture Overview
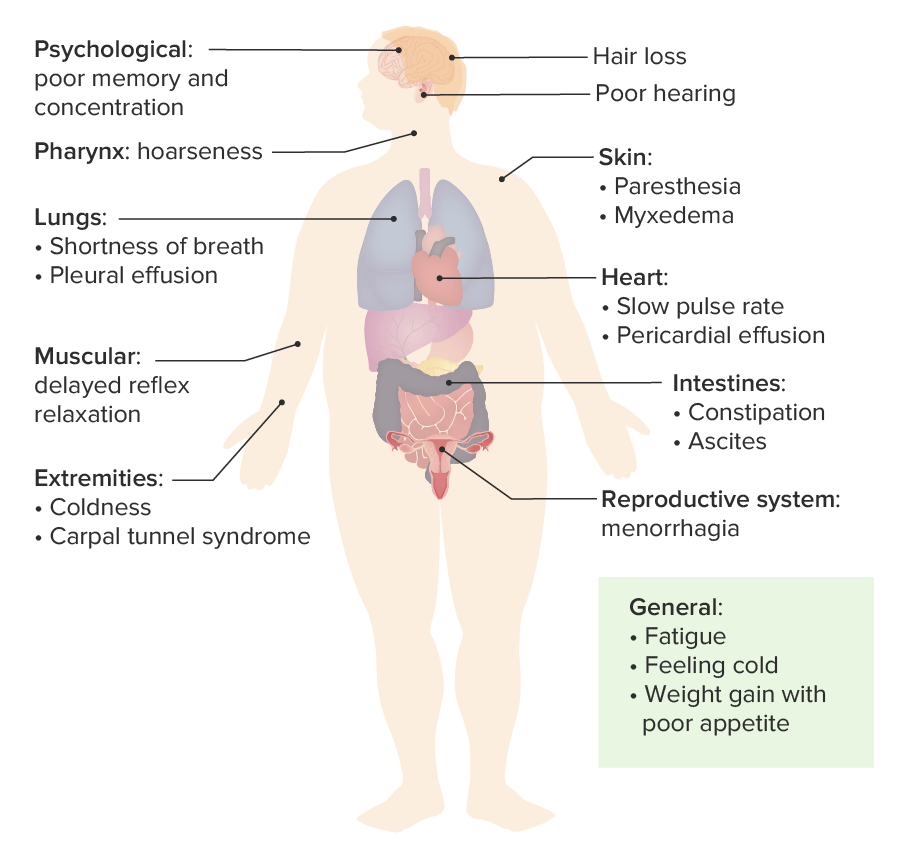
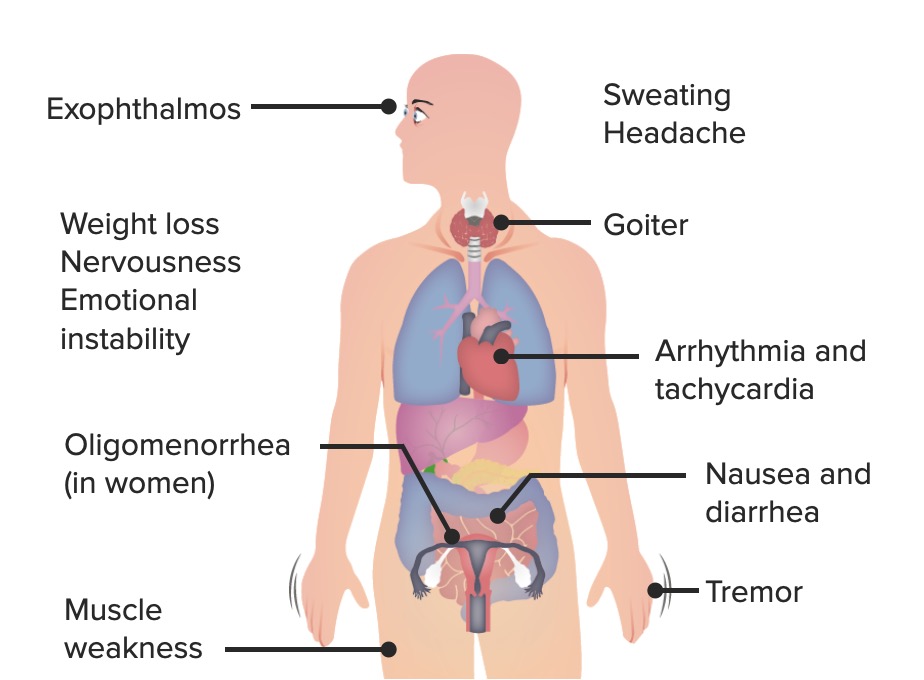
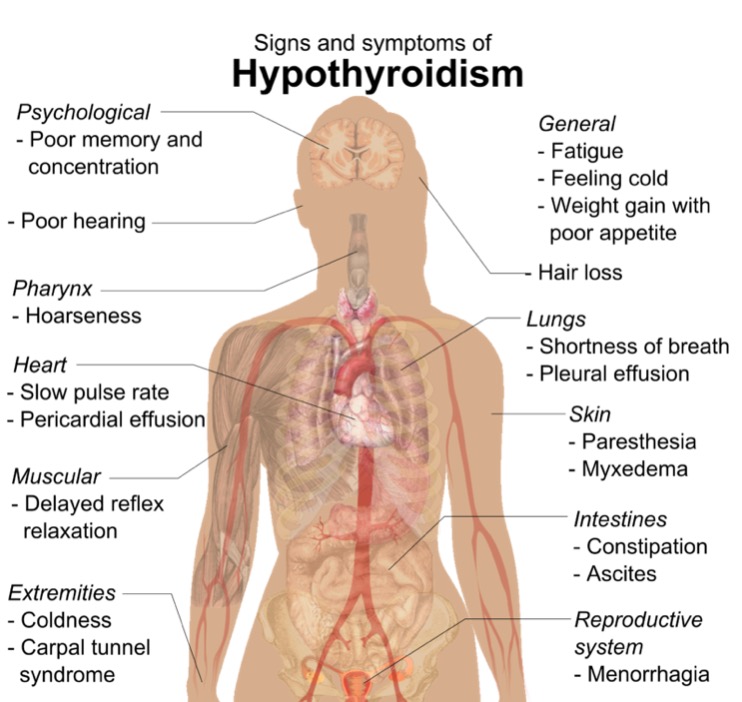
00:01 Causes of metabolic neuropathy. 00:03 Diabetes is always on top of that list as is thyroid disease. 00:07 Hepatic failure, your kidneys' failing, uremic neuropathy. That's an important one. 00:14 At the end of this entire section, I wanna walk you through a very, very important, what I call a polyneuropathy nirvana diagram, as we shall see. 00:25 Porphyric neuropathy. What does that mean? You know about -- by chemistry. 00:31 Did you know about your porphyria pathway on your way to produce your heme? And in that porphyria pathway, there are a couple of diseases or biochemical pathologies as you should be familiar with. 00:43 One of them being acute intermittent porphyria. 00:46 Vitamin deficiencies, either B1, B6, or B12. 00:50 Once again, remember B1, that's a problem, thymine. 00:54 B6 require for once again, proper myelination and of course B12. 01:00 Critical care neuropathy. These are metabolic neuropathies. Important ideologies. 01:05 Let's quickly walk through diabetic neuropathy. 01:09 Chronic, progressive, distal, symmetric diabetic polyneuropathy. 01:13 Every single one of there, incredibly important. 01:17 Diabetes in the US, type II diabetes of course, extremely common. 01:22 Chronicity, decades have gone by, and now at this point, you're gonna have symmetric and distal neuropathy taken place. 01:32 Don't we? Most common presentation: small and large fiber involvement. 01:37 Neuropathic pain is usually prominent. 01:40 For example, what about the nerves in the stomach? Would they be lost? Well, absolutely. So, you have paralysis of the stomach. We call this gastroparesis. 01:49 Or maybe your patient has suffered a myocardial infarction and there is no chest pain. 01:54 A silent myocardial infarction. Nerves have been lost. 01:58 Or down in the feet and here once again, the nerves. 02:04 You're worried about decubitus ulcers, aren’t you? The diabetic neuropathy, small, large fibers. 02:09 Neuropathic pain, usually prominent. 02:11 If you're actually wondering about what's happening to your nerves. 02:15 Clinical features. Initial symptoms are severe thigh and back pain with diabetic neuropathy and with diabetic proximal motor neuropath is what we're referring to specifically or diabetic glutinous amyotrophy. 02:31 Followed by hip and thigh muscle weakness and atrophy so you begin initially with thigh and back pain and then followed by hip and thigh muscle weakness and atrophy. 02:43 You put all this together and you call it amyotrophy. Proximal motor. 02:48 We have the diabetic proximal motor neuropathy. 02:53 Continuing with our discussion, acute axonal diabetic polyneuropathy and then with diabetes, remember there's no discrimination here and by that, I mean you could have diabetic mononeuropathy. What's that mean? You could have one nerve that is being affected. 03:09 Maybe radial nerve, maybe the ulnar nerve, maybe the median nerve, maybe the common peroneal nerve. 03:14 You could have the nerves coming out of the spinal cord, radiculopathy, polyradiculopathy, compression neuropathy. 03:24 All are significantly much more common in patients that are diabetic. 03:28 Every single nerve just about in a patient with diabetes over a long period of time, if not properly managed, is at risk for injury. 03:38 Plain and simple. To a pathologist, maybe. Through a doctor, possibly. 03:44 But for the patient, it's a lot of education, isn't it? Management. Well, the most important thing is going to be glycemic control. 03:54 That's your best measure of treatment, and by this we mean what? Lifestyle modification: lose weight, watch your diet. 04:01 And why do I roll my eyes when I do that, because you know, if you've done your rotations or for those of you that are practicing, it's easier said than done. 04:10 The symptomatic management. 04:12 Well, now if you're actually getting into diabetic neuropathy, you need to treat the symptoms. 04:19 Antidepressants. Antiepileptics, especially carbamazepine and perhaps gabapentin. 04:25 Remember carbamazepine? It was actually a first-line drug for trigeminal neuralgia so we know that carbamazepine definitely helps out with people that have neuropathies. 04:35 Tramadol. Opiates, maybe perhaps because of refractory cases. 04:41 The pain is actually intolerable sometimes and -- oh, this is a deadly road, isn't it? The opioid, huge discussion, behavioral science. 04:49 And NSAIDS for entrapment neuropathies as well.
About the Lecture
The lecture Metabolic Neuropathies and Diabetic Neuropathy by Carlo Raj, MD is from the course Polyneuropathy. It contains the following chapters:
- Metabolic Neuropathies
- Diabetic Neuropathy
Included Quiz Questions
A 50-year-old African American man with a long-standing history of type 2 diabetes mellitus and hypertension presents to your office with numbness and weakness in his legs. What is the most likely diagnosis?
- Metabolic neuropathy
- Uremic neuropathy
- Porphyric neuropathy
- Critical illness neuropathy
- Vitamin B6 deficiency
A 35-year-old woman presents to your office with weakness and numbness in her legs. She never had a medical check-up and complains that she develops a rash all over her body when exposed to the sun. What is the most likely diagnosis?
- Acute intermittent porphyric polyneuropathy
- Uremic polyneuropathy
- Vitamin B12 deficiency
- Thyroid disease
- Diabetic neuropathy
Which of the following is true regarding diabetic neuropathy?
- Distal and symmetric
- Involvement of small fibers only
- Involvement of large fibers only
- Proximal and asymmetric
- Neuropathic pain not prominent
Which of the following is NOT common in diabetic neuropathy?
- Neuromyelitis optica
- Compression neuropathy
- Acute axonal polyneuropathy
- Mononeuropathy
- Polyradiculopathy
Author of lecture Metabolic Neuropathies and Diabetic Neuropathy

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Clear emphasis was made, and the pace was easy for audience to follow
