Playlist
Show Playlist
Hide Playlist
Plaque Distribution and Athero-protective and Athero-prone Waveforms

-
Slides Atherosclerosis Risk Factors.pdf
-
Download Lecture Overview
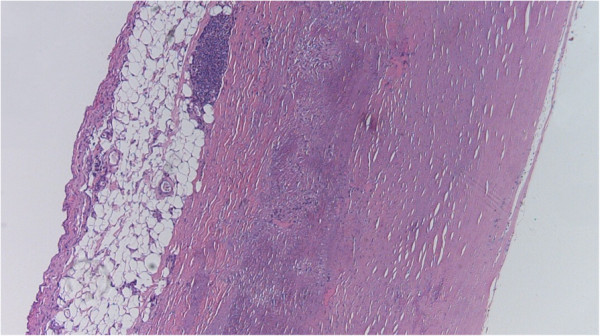
00:02 Another interesting point, in any vessel in the body, it has been exposed, theoretically uniformly, to all of the things that drive the production of atherosclerosis. 00:16 So if there is hypertension, the entire vascular tree is pretty much susceptible to that same level high blood pressure. 00:23 If there's hypercholesterolemia, pretty much the entire vascular tree susceptible or is being exposed to that same level of cholesterol. 00:32 If you are a smoker, whatever the evil humours are, that are in that cigarette smoke, that's also been distributed and exposed everywhere within the vascular tree. 00:43 And yet, when we look at atherosclerosis, it is not a uniform process. 00:50 That is to say, only certain parts of certain vessels are impacted. 00:55 It's a non random distribution. 00:58 So the lesion that are the.. 01:00 The image that we're looking at in the middle there, that has black, that's an aorta. 01:06 And we have taken the aorta out, and then labelled it with a compound called Oil Red O. 01:13 And that will stain lipid deposits in atherosclerotic plaque. 01:18 That red is only in certain areas. 01:21 It's not everywhere. 01:23 Even though this entire aorta was subjected to the same evil humours in cigarette smoke and hypertension, in diabetes all about. 01:33 The image on the far right is a coronary artery. 01:37 And the circle all the way around it is the typical medial smooth muscle of the normal arterial wall. 01:45 That kind of semi circle of pink that's in the upper two thirds of the vessel. 01:51 That's atherosclerotic plaque. 01:53 Note, that part of the vessel has atherosclerosis, the bottom part of the vessel is absolutely pristine. 02:00 It's thin walled, there's no athero. 02:03 And the difference between the top and the bottom were flow characteristics. 02:08 So that's the next thing I want to say, flow influences where plaque develops. 02:13 And in the image in the middle, you can see at branch points, particularly up again, around the arch vessels up near the top, where there's branching, there's a lot more athero. 02:23 And there tends to be more athero as we go more distal. 02:26 And at branch points, all that red, through the thoracic aorta, is because we have little tiny branch point vessels, and it's at those bifurcations, where we have turbulence, that we're getting atherosclerosis. 02:40 So it's not just all the other things we talked about, including not just inflammation, but it's also influenced by flow. 02:48 Let's look at this a little bit more closely. 02:50 Just because this is near and dear to my heart, no pun intended. 02:54 If we look at say the carotid bifurcation, so this is a model of the carotid bifurcation into the internal and external carotids. 03:03 We see that there are areas up near the top of that bifurcation where flow is now physiologically laminar at a certain pressure and flow rate. 03:13 And the flow is going in straight lines. 03:16 In that region of the bifurcation near the top where it's laminar flow, we tend not to get atherosclerosis. 03:26 If we look at this, and it's been modeled very carefully with MIT undergraduates and a lot of very interesting studies. 03:35 There's a certain flow characteristics. 03:37 Remember, this is pulsatile flow. 03:39 So you can have a heartbeat, and we're seeing the shear stress shown there as a function of time throughout the cardiac cycle. 03:46 The athero-protective waveform is tears your shear stress shows that particular waveform. 03:53 Now if we go and look at that same carotid bifurcation, and we look at a lower area, lower down, where we are more prone to get atherosclerosis, so it's athero prone, there is turbulence or low shear. 04:08 And the waveform looks quite different. 04:12 And we can actually model those waveforms in Vitro experiments. 04:19 So we can take endothelial cells and see show they behave if we give them an athero-protective shear stress waveform, or an athero prone shear stress waveform. 04:30 To really get at our hypothesis, that flow also determines where atherosclerosis develops. 04:37 That's what's shown here and this is just, this is a real experiment, but we'll walk through it. 04:44 So if we have a vessel shown on the right, and we have an inflammatory cell, a monocyte, flowing through that area, the endothelial cells have relatively flatter cells top and bottom. 04:56 The middle of that is the lumen in the thing with the white rim around it, it is a monocyte. 05:02 And if we don't have any endothelial cell treatment, there is no expression of adhesion markers, and we don't recruit inflammatory cells remember inflammation and major driver of atherosclerosis. 05:15 If we hit thate ndothelium with interleukin-1, a pro inflammatory mediator, then we will get some degree of VCAM, vascular cell adhesion molecule expression, and we will get some binding of monocytes. 05:31 And they will then crawl across and become macrophages. 05:33 And we'll start the inflammatory part of the atherosclerosis cascade. 05:39 Cool. 05:40 And that's what happens. 05:40 I mean, it's just inflammation driving that initial expression. 05:44 Now, if we do our different flows over the surface of the endothelial, what happens? So if we take interleukin-1, and an athero-prone, you can see that squiggle down the middle. 05:56 That's the athero-prone waveform, those endothelial cells become incredibly sticky. 06:02 Make lots and lots of vascular cell adhesion molecule, and we get lots, lots more of inflammatory cell recruitment. 06:10 Wow. 06:11 All we've changed here is Flow. 06:14 Now, you're thinking okay, now what happens if I take interleukin-1 and I have athero-protective waveform? We don't make any VCAM. 06:23 We do not recruit and activate those inflammatory cells. 06:28 So flow clearly also influences the development of atherosclerotic plaque. 06:38 With that, we've kind of looked at risk factors, traditional and not so traditional. 06:43 And we'll go on from there and look at what plaques look like.
About the Lecture
The lecture Plaque Distribution and Athero-protective and Athero-prone Waveforms by Richard Mitchell, MD, PhD is from the course Atherosclerosis.
Included Quiz Questions
What pattern does the development of atherosclerotic plaques follow?
- Nonrandom distribution
- Uniform distribution
- Predetermined distribution
- Systematic distribution
- Cumulative distribution
What influences the development of atherosclerotic plaques?
- Blood flow turbulence
- Blood viscosity
- Diameter of the vessel lumen
- Elasticity of the blood vessel
- Collagen in the vessel wall
What is the response of the vascular endothelium to interleukin-1?
- VCAM-1 expression
- Influx of CD4-positive/CD8-positive lymphocytes
- Transendothelial migration (TEM)
- Downregulation of CAMs (such as cadherins)
- Upregulation of TNF-alpha
Author of lecture Plaque Distribution and Athero-protective and Athero-prone Waveforms

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
