Playlist
Show Playlist
Hide Playlist
Penicillins – Cell Wall Synthesis Inhibitors (Antibiotics)

-
Slides Antimicrobial Pharmacology Penicillins.pdf.pdf
-
Download Lecture Overview
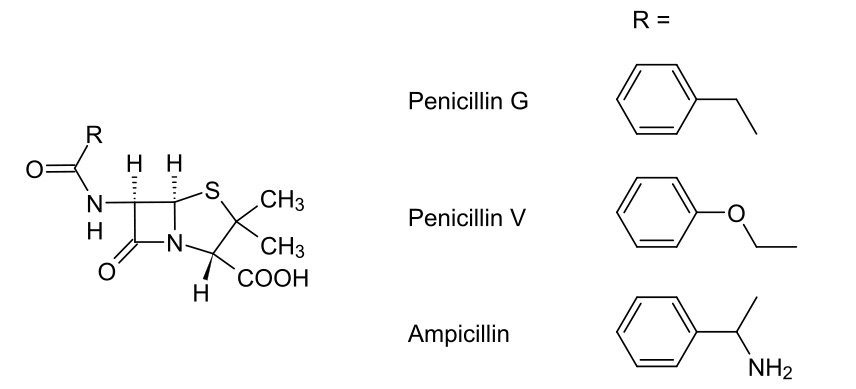
00:01 Now our cell wall synthesis inhibitors have different subtypes and I mentioned them before. Let's start off with the penicillins. 00:09 We have many different subcategories of the penicillins. 00:12 There are the natural ones, the beta lactamase resistance ones, the amino and the carboxy penicillins and then there's the ureido carboxy penicillins and the ureido penicillins. Now, penicillin is one of our oldest drugs. 00:25 The discovery of penicillin was one of the most significant medical breakthroughs of the 20th century. In 1928, Dr. 00:31 Alexander Fleming observed a mold, Penicillium notatum, contaminating his Petri dishes, which inhibited the growth of Staphylococcus aureus. 00:41 He could not identify the antibacterial element due to resource constraints and his findings initially attracted little attention. 00:49 Ten years later, in 1938, Dr. 00:52 Howard Florey at Oxford University saw potential in Fleming's work and successfully isolated and purified penicillin from the mold. 01:02 By 1940, Florey's experiments on mice infected with streptococcus showed that while untreated mice died, those treated with penicillin survived, marking a significant milestone. 01:14 Between 1941 and 1942, mass production of penicillin was realized. 01:19 In 1942, the first human patient was successfully treated with penicillin. During World War II, from 1942 to 1945, penicillin was initially reserved for Allied soldiers, significantly reducing the death rate from battle wounds and other infections, including bacterial pneumonia. 01:39 By 1945, it was released to the public as American companies were producing it in large quantities, and it was marketed as a treatment for various infections, including gonorrhea. 01:51 In 1945, the Nobel Prize was awarded to Fleming, Florey, and Chain for penicillin, with Fleming warning of possible bacterial resistance. 02:01 Dr. Norman Heatley, also pivotal in its development, was later acknowledged by Oxford with an honorary doctorate of medicine. 02:09 There are several different types of penicillins. 02:12 The natural penicillin are just what they sound like, they come from the penicillium mold. 02:19 Penicillin G is the most commonly known but there's many different types, there's K, N, V, so the narrow spectrum penicillin G is used mostly in strep throat and necrotizing enterocolitis. 02:34 These agents are very commonly used in syphilis and leptospirosis and they are of course used in gonorrhea but not so much anymore. 02:43 This is an old drug and it tended to focus mostly on gram positive organisms and it was given intravenously or intramuscularly. 02:51 Nowadays, we have newer agents that have mostly replaced penicillin G but it's still used quite a bit in certain areas and in certain countries. 03:01 Penicillin V on the other hand is used a little bit more commonly in strep throat. We also use it in otitis media especially in children. 03:09 We use it sometimes in cellulitis and of course we use it to decrease the risk of rheumatic fever. We do use it in splenectomy patients because splenectomy patients are more prone to certain types of bacterial infections. 03:24 One of the nice things about penicillin V compared to G is that it's acid stable. 03:28 That means it can survive in the gut and therefore can be given orally. 03:34 The next category consists of beta-lactamase resistant penicillins. 03:39 Now they tend to be narrow spectrum as well. 03:41 They can include methicillin or oxacillin. 03:44 I've highlighted two of them that are most commonly used in bold face. 03:48 Cloxacillin is something I literally just prescribed a few days ago. 03:53 It's used in skin infections cellulitis, impetigo. 03:56 It's also used in some pneumonias, septic arthritis and otitis. 04:02 Now it is safe in pregnancies so we tend to use it a lot in our pregnant patients particularly those with skin infections or with otitis infections. 04:11 Staph that produce beta-lactamase can be treated with cloxacillin. 04:16 Now there is a long R chain that is present in cloxacillin. 04:21 This prevents the beta lactamase from actually binding to it that's why it's so effective even in patients who have beta lactamase producing bacteria. 04:31 Methicillin is another drug in this category. 04:35 It isn't really used as much anymore. 04:38 It is important because we know about a lot of resistance to this drug so we have typically methicillin resistant staphylococcal aureus. Now MRSA as its commonly known is a real problem in our hospitals. So I mention methicillin not because we use it but because we shouldn't use. It is also linked to interstitial nephritis that's an important exam question for some of you but as I've said again, we don't really use this medication anymore. Another medication that we use in this class is nafcillin. It is associated with neutropenia, I won't really go into too much detail other than the fact that nafcillin neutropenia, there's a memory cue their N and N and I have seen that in exam questions as well. Okay, let's move on to the amino penicillins. 05:29 Amino penicillin includes ampicillin and amoxicillin and I bet that you have probably been on one of these antibiotics. 05:38 They have a wide spectrum of activity but they can still be susceptible to the beta lactamases. 05:45 They can be oral or they can be intravenous or they can be intramuscular. 05:50 We use these drugs in various infections that includes bacterial meningitis, endocarditis, GI infections like salmonella. 06:00 They can also be used in genitourinary infections and they can often be used in catheter-based infections. 06:07 For example, I had a patient in the nursing home that I see that I round in had a catheter-based infection of his indwelling urinary catheter. 06:16 We use a combination of ampicillin and gentamycin to treat the infection so it's a very, very, commonly used class of drugs. 06:24 We also use ampicillin and amoxicillin in bacterial endocarditis prophylaxis. What is bacterial endocarditis prophylaxis? If you have an implanted cardiac valve, let's say an artificial aortic valve and then you go for a dental surgery. 06:41 You need to have antibiotics to protect the valve from becoming infected so we use a ampicillin as a gram taken a half hour before the procedure and that usually protects that patient from getting infected from his dental surgery. Ampicillin can also be enhanced with additional agent so amoxicillin or ampicillin can be added with clavulanate to protect it from the effects of the beta-lactamase and also give it added synergistic activity. 07:14 In enterococcal infections we use aminoglycosides in combination with the ampicillin or the amoxicillin. 07:22 As I've mentioned before, ampicillin gentamycin is a very common type of regimen that we use for complicated infections. 07:31 Next, we have the carboxy penicillin these include like ticarcillin. 07:35 Now ticarcillin is generally considered to be more of an intensive care unit drug. It has strong activity against gram negative organisms so we will sometimes use carboxypenicillins against pseudomonas and maltophilia type infection. 07:51 We will also use it in combination with the aminoglycosides. 07:56 We almost always take these medications in combination with clavulanate so for example we'll have ticarcillin clavulanate as a combination product because we want to protect against resistance. 08:11 Finally, we have the ureidopenicillins. 08:14 The ureidopenicillins can include drugs like pipercillin. 08:18 Pipercillin Is also an intensive care unit kind of a drug. 08:21 It’s a very broad-spectrum agent it has very good gram-negative coverage but it also has some good gram-positive coverage as well. 08:29 Once again, we like to pair this with a beta-lactamase inhibitor. 08:33 In the case of piperacillin, we combine it with tazobactam. 08:38 Pseudomonas is a problematic agent that we sometimes see in wet infections, so we often call this the sneaker shoe kind of infection, it smells like sneaker shoes just that horrible kind of a stench. 08:52 We see that sometimes in intubated patients in the intensive care unit complicated infections involving areas like mucosa, so it's typically thought of as a wet infection and piperacillin is often use to treat it. Now, one of the problems of piperacillin of course is that it lacks strong activity against staph aureus so that can be a problem when you are trying to choose a medication or an antibiotic regimen and you don't know what the cause of the organism is or you don't have a good suspicion. 09:24 We also use piperacillin tazobactam in neutropenic sepsis so like I said it's a very good antibiotic in very sick patients. 09:34 Mezlocillin is another one that I think is important to remember because it is excreted by the liver. Now why is that important? Why do we want a drug that's actually excreted by the liver, and why would that give us any kind of advantage? Well, think about this, if you have a biliary tract infection in the liver it makes sense to give a drug that's concentrated in the liver, that's where we use this medication.
About the Lecture
The lecture Penicillins – Cell Wall Synthesis Inhibitors (Antibiotics) by Pravin Shukle, MD is from the course Antimicrobial Pharmacology.
Included Quiz Questions
Which of the following antimicrobial agents has the strongest activity against gram-negative organisms?
- Piperacillin
- Ampicillin
- Amoxicillin
- Methicillin
- Nafcillin
Which statement about penicillins is FALSE?
- Ticarcillin is contraindicated with administration of aminoglycosides.
- Methicillin is associated with interstital nephritis.
- Nafcillin is associated with neutropenia.
- Ampicillin is a wide spectrum antibiotic that is susceptible to beta lactamases.
- Oxacillin is a narrow spectrum penicillin.
Methicillin-resistant Staphylococcal aureus (MRSA) is...?
- ...resistant to all penicillins.
- ...commonly treated with amoxicillin.
- ...sometimes sensitive to methicillin.
- ...always susceptible to ceftriaxone.
- ...responsive to treatment with penicillin G.
Author of lecture Penicillins – Cell Wall Synthesis Inhibitors (Antibiotics)

Pravin Shukle, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Thanks for the lecture, but I have a question regarding gram + bacterias, isn't Neisseria Gonorrhea the flora that causes gonorrhea ? to my knowledge it's a diplococcus and it's gram-negative, does it means that penicillins are also like similar in action just like cephalosporins especially the third generational ones?
enjoyed the lecture, I would love one on the legalities of pharm and the laws for prescribing
