Playlist
Show Playlist
Hide Playlist
Non-Traumatic Abnormalities of the Spine


-
Slides Non Traumatic Abnormalities of the Spine.pdf
-
Download Lecture Overview
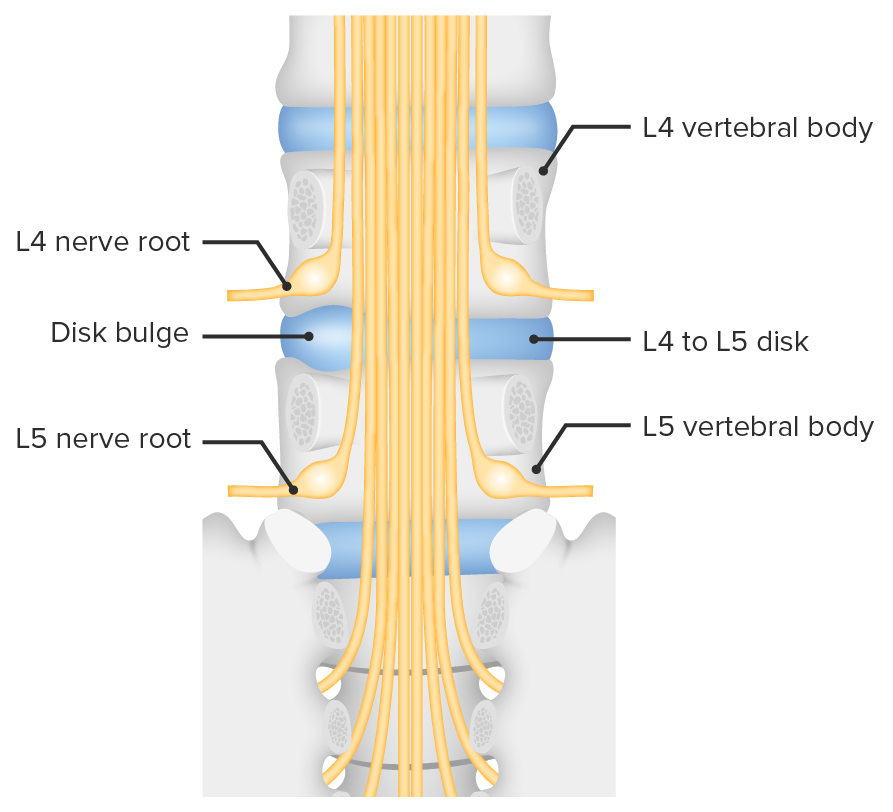
00:01 So in this lecture we'll be discussing spinal imaging. 00:04 MRI's usually the best method of choice to image the spine. 00:09 However, as you know, MRI has a very long acquisition time so because of their speed of acquisition and easy availability radiographs are usually used as the first line. 00:18 CT is also often used to detect bony abnormalities and to evaluate for spinal trauma. 00:23 So the spine should be normally aligned and the way to assess the alignment is to look at these 3 lines. 00:30 There are 3 lines that should run parallel and smoothly along the spine to help you exclude malalignment. 00:36 The first line is the anterior longitudinal line which is the white line that you see here. 00:41 There's the posterior longitudinal line which is the solid black line and then the last line is the spinolaminar line. 00:48 So when you're looking for malalignment always look at these 3. 00:52 Let's discuss the vertebral body anatomy a little bit before we get into the pathology. 00:57 So this is the normal anatomy of the vertebral body. 01:00 You have the actual body of the vertebra here. 01:03 You have the pedicle, posteriorly you have the lamina on both sides, you also have the spinous process posteriorly. 01:12 On each side you have a transverse process and then the center here is the spinal canal. 01:17 So you should take a look at each of these portions when you're taking a look at the vertebral body to ensure that there isn't a subtle fracture of any of these locations. 01:25 This is a 3D rendering that was based off of the CT of a vertebral body at a different level. 01:31 So here you have the actual body again and you have the transverse foramen which we didn't see on the previous one. 01:38 You also have a superior articular facet which articulates with the vertebral body above it. 01:43 And then again posteriorly we have the spinous process. 01:46 So the neural foramina are openings within the vertebral bodies through which the nerve, the blood vessels, and the fat traverse. 01:55 Let's take a look at frontal radiographic anatomy. 01:59 So here in the midline we have the spinous processes and you wanna ensure that they stay in midline. 02:05 If the patient is rotated this can help make it a little bit difficult to take a look at the spine. We have the facet joints right here and then the round circles on either side are the pedicles. 02:19 When you do a radiograph of the spine, you often take a postural oblique image as well because it helps you delineate the anatomy a little bit better. 02:28 You might have heard of the scotty dog, so as you can see here this is an outline of what the scotty dog looks like. 02:34 So let's take a look at the scotty dog here. 02:37 So again, let me outline it for you right here and then let's take a look at what each of the portions of the dog represent. 02:44 So here we have the ear which represents the superior articular facet. 02:48 The nose represents the transverse process. The eye represents the pedicle. 02:55 The neck represents the pars interarticularis and the foot represents the inferior articular facet. 03:03 This is actually a good view to take a look at the pars interarticularis which you don't see that well on the other views. 03:09 Patients often have a congenital pars defect and its well seen on this view. 03:13 So let's take a look at spinal anatomies seen on MRI. 03:18 So here, we have a T1 weighted image and then here we have a T2 weighted image. 03:22 On the T2 weighted image the CSF is bright as you would expect and you can see that the lumbar spine is labeled here. 03:30 When you're taking a look at an MRI of the lumbar spine or even the thoracic spine, it's actually helpful to ahead and label the vertebral bodies first because it can help you identify the findings a little bit better. 03:41 The spinal cord usually ends at about the L1/L2 level and this is called as the conus and the discs are well seen on MRI here. 03:50 So there are 7 cervical vertebrae. 03:56 There are 12 rib-bearing thoracic vertebrae and there are 5 lumbar vertebrae. 04:01 There are about 5 fused sacral vertebrae in every patient. 04:05 In terms of the nerve roots from about C1 to C7, the nerve roots exit above their respective vertebral body. 04:13 There's actually a C8 nerve root which enters between the C7 and T1 vertebral body and then the remaining nerve roots exit below their respective vertebral bodies. 04:23 So this comes into play when a patient comes in with neurological symptoms and you see a compression of the transverse foramen and then you wanna see which level of this is going to affect. 04:32 So a disc herniation is bulging of the disc material and is usually caused by degeneration of the outer annular fibers of the disc. 04:40 It usually occurs in the lumbar spine and it often causes back pain. 04:45 It's actually one of the most common reasons a patient presents with back pain. 04:49 Disc herniations in the cervical spine usually result in radiculopathy and the symptoms are due to compression of the nerve roots. 04:57 So let's go over a little bit of herniation terminology. 05:01 A disc bulge as you can see in this image is diffused bulging of the disc from all sides. A disc herniation, however, is a focal disc bulge which is then divided into a protrusion and extrusion. 05:13 So protrusion is when the disc material herniates through but it remains in contact with the parent disc and it appears wider than tall. 05:24 So as you can see here, this is an example of a protrusion and it's wider in this direction than it is tall. 05:30 An extrusion is disc material that herniates through and appears taller than wide. 05:36 As you can see here, this is an example of an extrusion right here and this is taller than it is wide. 05:44 A sequestration is a disc material that herniates through and actually detaches from the parent disc as you can see here. 05:52 This is an example of an L5-S1 disc herniation, seen on a sagittal view of the lumbar spine. 06:00 So you cans see here the disc and you can see it herniating through back here. 06:05 This is an example of a normal disc that doesn't protrude at all into the spinal canal. 06:10 So you can have different types of degenerative changes that occur within the spine. 06:17 You could have degenerative disc changes or you could have facet degenerative changes. 06:22 So dehydration of the disc is what results in degeneration of the disc. 06:29 It causes loss of the height of the disc space and it causes a decrease in the T2 signal intensity as seen on MRI. 06:36 You also see sclerosis of the endplates and you may see marginal osteophytes. 06:41 And it can also cause what's called the vacuum phenomenon, which is release of nitrogen gas from the disc causing air density within the disc spaces. 06:50 So this is a radiographic example of degenerative disc disease. 06:54 So here we have loss of the disc space. 06:56 We have endplate sclerosis at each of the vertebral bodies surrounding this area of degeneration and you have vaccum phenomenon so if you look right here you have a little bit of gas within the disc space and that's from the nitrogen gas that's released out of the disc. 07:12 So facet joints are true synovial joints. 07:16 You also have uncovertebral joints which are also synovial joints between the C3 and T1 vertebral bodies. 07:22 So they are localized to that portion of the spine and both of these can undergo degenerative change. 07:27 So degenerative changes are noted here at both the facet and uncovertebral joints and you can see small marginal osteophytes protruding into the neural foramen. 07:40 This patient also has degenerative disc disease and you can see that by the disc space narrowing and the anterior marginal osteophytes. 07:47 So you have a little bit of narrowing at this level, you also have a little bit of narrowing at this level and they are relatively large marginal osteophytes at multiple levels here. 07:56 This can actually result in spinal canal and transverse foraminal narrowing which can then cause pain due to nerve compression. 08:03 So a compression fracture is the most commonly found fracture within the spine. 08:09 It's usually the result of osteoporosis and it often involves the anterior and superior aspect of the vertebral body and it causes a wedge shaped deformity as you can see here. 08:19 So this is the anterior aspect of the vertebral body, you have a compression fracture here and you can see narrowing of the anterior aspect of the vertebral body which is more narrow than the posterior is. 08:30 This can also be caused by trauma or malignancy. 08:33 This is an example of a patient with a compression fracture in the thoracic spine. 08:39 You can see here the patient likely has osteoporosis. 08:43 The bones look a little bit demineralized and then if you take a look at a normal vertebral body you can see that the one right here is actually compressed, so this is an example of a compression fracture and in this patient, which happens relatively frequently, this has resulted in increased thoracic kyphosis. 08:59 So vertebral metastasis are the most common kind of malignancy that's found within the spine and usually this come from the lung or the breast. 09:10 They can cause destruction of the vertebral body, they can cause a compression deformity and this can include the entire vertebral body including the posterior aspect and this one way of differentiating whether a compression is due to a malignancy or whether it's due to osteoporosis. 09:24 The osteoporotic compression deformity is usually involved just the anterior aspect of the vertebral body. 09:29 Spinal cord metastasis themselves are actually exceedingly rare. 09:33 The malignancy usually goes to the vertebral bodies. 09:36 So you can have an osteoblastic or an osteolytic malignancy. 09:40 An osteoblastic malignancy is one that is bone producing and will appear sclerotic. 09:45 An osteolytic malignancy is one that's bone destroying and will appear lucent. 09:50 Bone scans are actually the best way of examining for vertebral metastases. 09:55 So this is a nuclear medicine study if you remember and it's highly sensitive in detecting spinal malignancy. 10:00 You can see abnormal uptake in areas of bony production but lytic met actually may not show increased uptake and can be missed. 10:08 MRI's also highly sensitive but it's not usually used as a screening exam because it's very expensive and very time consuming. 10:16 A vertebral malignancy usually presents as a T1 hypointense lesion and a T2 hyperintense lesion. 10:23 After contrast, this usually enhance, so let's take a look. 10:28 So we have T1 and T2 weighted MRI images here. 10:32 So as you can see on the T1 weighted images, the vertebral bodies are slightly bright in appearance or hyperintense. 10:39 On the T2 weighted images, the vertebral bodies are slightly hypointense. 10:44 However, we have 1 vertebral body here that appears different than the others. 10:49 So this one is actually hypointense on the T1 weighted images and hyperintense on the T2 weighted images. 10:56 This actually represents a metastasis from the patient's known breast cancer. 11:00 So we've gone over some normal anatomy of spinal imaging and we've gone over some things that you wanna look for when you take a look at a spinal exam either radiographically or by MRI.
About the Lecture
The lecture Non-Traumatic Abnormalities of the Spine by Hetal Verma, MD is from the course Neuroradiology. It contains the following chapters:
- Spinal Anatomy
- Disc Herniation
- Spinal Malignancy
Included Quiz Questions
Which of the following is NOT true regarding spinal malignancy?
- Spinal cord metastasis is the second most common cause of spinal malignancy.
- Vertebral metastasis is the most common malignancy found in the spine.
- Lung and breast carcinoma are the most common cause of spinal malignancy.
- The vertebral metastasis results in the destruction of the vertebral body.
- It results in compression deformity involving the entire vertebral body including the posterior aspect.
Which statement is FALSE regarding spinal imaging?
- MRI is usually the first line of diagnostic imaging.
- MRI is the best method to image the spine.
- CT is often used to detect bony lesions and for spinal trauma.
- In a normal radiograph, the anterior longitudinal line, posterior longitudinal line, and the spinolaminar line should run parallel to exclude malalignment.
- On CT, the superior articular facet articulates with the vertebral body above it.
What part of the "Scottie dog" corresponds to the transverse process in a posterior oblique radiograph?
- Nose
- Eye
- Neck
- Foot
- Ear
Disc herniation…
- …in the cervical spine often results in radiculopathy.
- …is due to the multiplication of the outer annular fibres of the disc.
- …is the shrinking of the disc material.
- …occurs most commonly in the thoracic spine.
- …results in scoliosis.
An x-ray of the lumbar spine to evaluate low back pain in a patient shows sclerosis of the endplates and marginal osteophytes. What is the most likely cause?
- Degenerative disc changes
- Disc protrusion
- Disc sequestration
- Fracture of the vertebral body
- Disc bulge
What is the most common complication of osteoporosis in the spine?
- Compression fracture
- Malignancy
- Disc bulging
- Disc degeneration
- Disc protrusion
Author of lecture Non-Traumatic Abnormalities of the Spine

Hetal Verma, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
All the needed information in a nutshell. To assess for spinal pathology "the Winking owl sign" can also be added. It is usually a sign of bone metastasis.
