Playlist
Show Playlist
Hide Playlist
Spontaneous Intracerebral Hemorrhage (ICH): Examination & Diagnosis

-
Emergency Medicine Bord Intracranial Hemorrhage.pdf
-
Download Lecture Overview
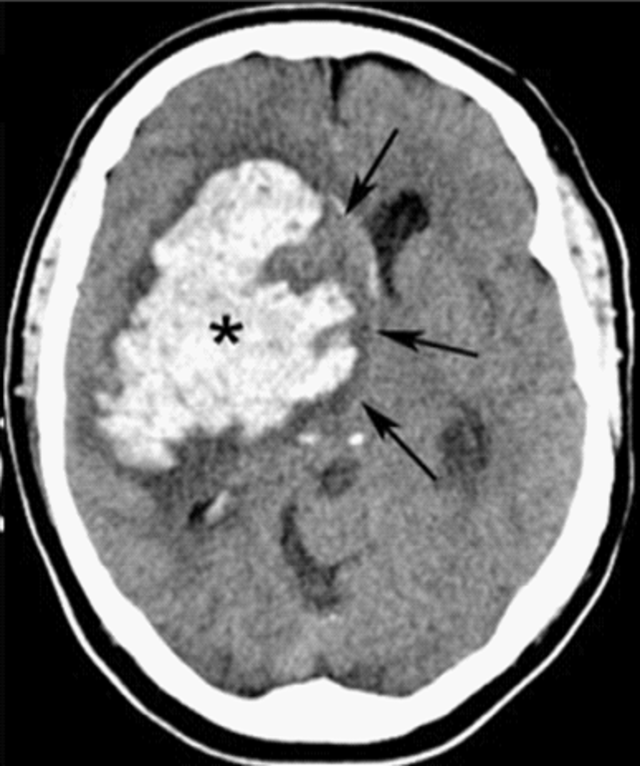
00:01 On the physical exam, you wanna make sure you do a careful neurologic exam. 00:05 In those initial phases, you wanna start thinking about your NIH stroke scale because sometimes this can be hard to differentiate from an ischemic stroke. 00:13 You wanna calculate a GCS score. 00:17 So the GCS stands for Glasgow Coma Score and it’s based on whether or not the patient has appropriate eye movements, appropriate speech, and an appropriate motor exam. 00:27 The scores on that range from three which is essentially a patient who’s unconscious with no movement, all the way to 15, which is a normally functioning person. 00:36 And then you wanna focus on the airway and breathing. 00:40 In Emergency Medicine, we’re always thinking about our most critically ill patients. 00:44 These patients actually may require intubation, so they might require a ventilatory support if they’re not able to breathe effectively, and especially in those bleeds that affect the brainstem, those patients may most definitely be altered and may require these additional steps. 01:01 So always while we’re performing our neurologic exam and calculating our GCS, we always wanna make sure that in the forefront of our brains, we’re focusing on the airway, breathing, and circulation component. 01:13 Now, when patients present with these symptoms, we definitely wanna make sure we’re thinking about the most dangerous things. 01:21 And one of the most dangerous things is intracerebral hemorrhage. 01:24 But we also wanna make sure that we’re keeping our differential diagnosis a little bit broad. 01:29 That we’re making sure we’re considering and thinking about other things that could explain this patient’s presenting symptoms. 01:34 Hypoglycemia is one of those. 01:36 A low blood sugar can present with a whole slow of different symptoms. 01:40 So keeping that on the differential and checking a finger stick. 01:44 Migraine headaches can present with some symptoms like this as well especially with the headache component. 01:50 Seizures can present with confusion especially in the post ictal period, the period after the seizure. 01:57 Tumors or mass legions, and then hypertensive encephalopathy. 02:03 Hypotensive encephalopathy is different than hypertensive vascular apathy. 02:08 Hypertensive vascular apathy is chronically elevated blood pressure that affects and weakens the vessels, whereas hypertensive encephalopathy is acute elevated blood pressure, which results in brain edema. 02:20 This is due to end organ damage, and this is a type of hypertensive emergency. 02:25 So for these patients, first and foremost, check a finger stick to rule out hypoglycemia as the cause here. 02:33 Then you wanna get an emergent head CT. 02:36 This is a non-contrast head CT. 02:38 So you wanna obtain it without giving any contrast in the IV and what this does is it helps to distinguish or differentiate between an ischemic process and a hemorrhagic process. 02:49 Acute blood, so blood that has been there relatively recently will appear bright white as it does on this head CT scan. 02:56 And all acute blood will appear that way when you’re getting that non-contrast head CT. 03:00 Over a period of time, it can get a little bit trickier because as time goes on, that blood takes on more of a greyish appearance and can actually really blend in with the brain tissue. 03:10 So you wanna make sure especially in those earlier scans, you’re looking for something that’s gonna light up bright white, similar to the color of what the bone looks like. 03:18 You wanna get coagulation studies. 03:19 Those are important for all patients but especially for patients who are on anticoagulation medications and you wanna try and ascertain that information when you’re getting the history from the patient or their family member, or the medics. 03:32 And then a toxicologic screen can sometimes be of benefit if a patient potentially used cocaine or another sympathomimetic.
About the Lecture
The lecture Spontaneous Intracerebral Hemorrhage (ICH): Examination & Diagnosis by Sharon Bord, MD is from the course Neurologic and Psychiatric Emergencies.
Included Quiz Questions
Which of the following is NOT an appropriate step in the initial evaluation of a patient with acute intracranial hemorrhage?
- Brain computed tomography scan with intravenous contrast
- Calculation of the Glasgow coma scale
- Finger stick glucose measurement
- Measurement of blood pressure
- Assessment of the airway
How does acute blood appear on a non-contrast head CT scan?
- Bright white
- Isodense with ventricles
- Isodense with brain parenchyma
- Hypodense
Author of lecture Spontaneous Intracerebral Hemorrhage (ICH): Examination & Diagnosis

Sharon Bord, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
