Playlist
Show Playlist
Hide Playlist
Increased Intracranial Pressure: Introduction

-
Slides 05 IncreasedIntracranialPressure Neuropathology I.pdf
-
Download Lecture Overview
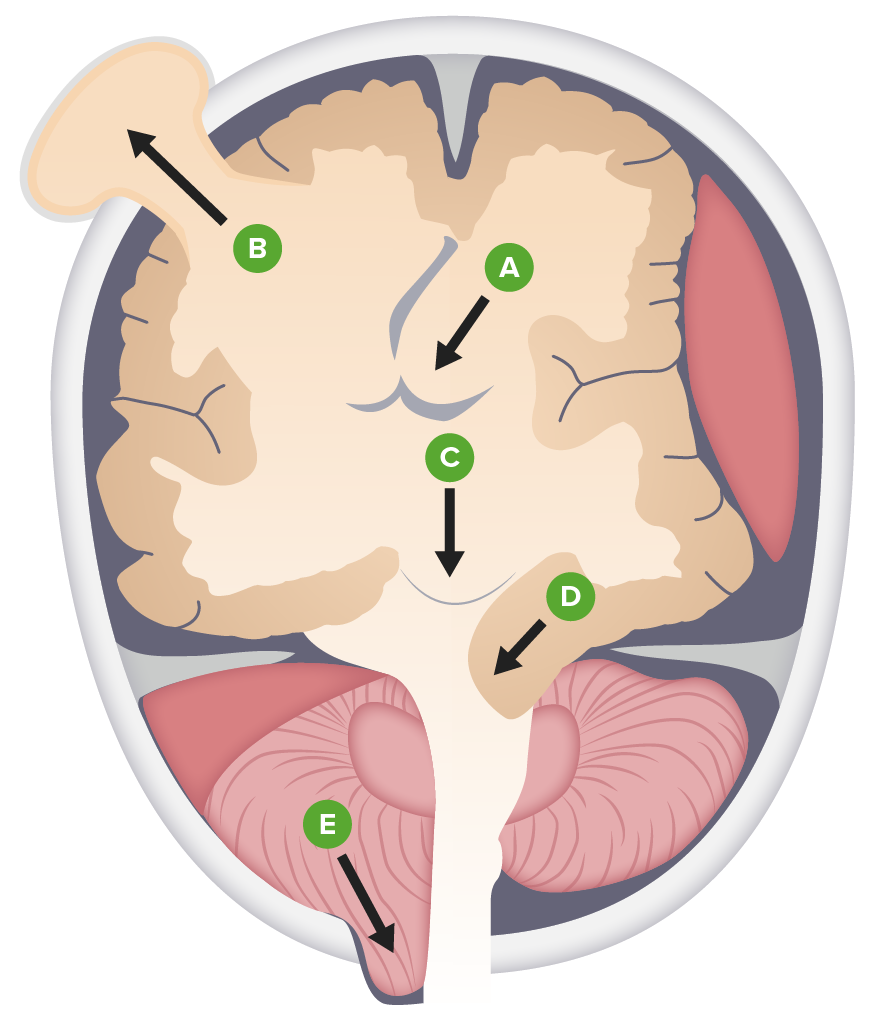
00:01 Let's take a look at increased intracranial pressure. 00:04 There are many ways in which intracranial pressure could be increased and we've discussed this a few times. 00:11 For example, if there's any type of hydrocephalus that could be an increase in intracranial pressure. 00:16 There are a few other important topics that we have to have to take a look at, including herniation, resulting in once again increase in intracranial pressure. 00:24 So there's a long list of differentials, but here, let's organize our thoughts and take a look at what happens. 00:32 We have something called a Monroe doctrine, a "brain in a box". 00:37 So in other words, let's say that you have the box, which is then increasing the pressure due to what ever reason in the brain, increasing its pressure. 00:48 The skull of course contains the brain, the CSF and the blood. 00:51 And so therefore, any one of those, in which it's undergoing, let's say, encephalitis and brain-type of space-occupying lesion. 00:59 We talked about hydrocephalus or perhaps even subarachnoid hemorrhage with blood. 01:04 All of this could result in increase in intracranial pressure. 01:17 Then increase in pressure then displaces something, doesn't it? And that something that it displaces is going to result in whatever symptoms that your patient is going to experience. 01:28 And here, let's say that our patient, Remember we talked about subarachnoid hemorrhage and we talked about hydrocephalus. 01:38 And with hydrocephalus, at some point in time, if it's left untreated, don't you think it's once again going to displace something? And that something that it displaces may then result in a herniation. 01:52 And that herniation is of different types. 01:57 And all of this, of course, is going to contribute to that already existing increased intracranial pressure. 02:04 In terms of increased intracranial pressure, think of this as being kind of like a topic like headache, where there's a list of differentials. 02:14 The same thing can be applied here as well. 02:16 Now, herniation occurs when focal or global pressure forces portions of the brain into the wrong spot. 02:23 So what are these different types of herniations that you want to be extremely familiar with? You want to know about subfalcine herniation. 02:33 Don't memorize this. 02:34 What does sub- mean? Underneath. 02:36 What is falcine referring to? The falx cerebri. 02:41 And for whatever reason, at some point in time, we'll talk about hematomas as well, right? When we talk about hematomas, epidural or you had your subdural, so you can have those types of hematomas. 02:53 So remember please that you could have a trauma resulting in hematoma and also at the same time, there could be displacement of the brain parenchyma in the wrong spot. 03:06 So imagine now, you're at your medial hemisphere of the brain and you just got hit by a baseball. 03:12 Boom! And now, you resulted in, let's say, an epidural hematoma. 03:18 In addition, let's say that the medial hemisphere of the brain is now moving underneath the falx, subfalcine, to the wrong spot, to the other side. 03:30 Guess what's going to happen? Continue with your story. 03:33 What story? What's the name of a blood vessel that is supplying the medial hemisphere of the brain? Aha! Anterior cerebral artery, right? Anterior cerebral artery. 03:45 And the medial hemisphere of the brain is supplying what part of the body? Is it my face or is it the lower extremity? Lower extremity. 03:58 So with the subfalcine herniation, it could result in lower extremity issues. 04:04 Clear? It's all a story. 04:06 All that you're doing from neuroanatomy is memorizing the facts so that you can apply the proper pathology and the disease so that you'd tell a story. 04:15 Otherwise, you're wasting your time. 04:18 What about uncal herniation? What does uncal refer to? The uncus. 04:23 Where is that? Oh yes, anatomy. 04:26 Temporal, good. 04:27 So another name for your uncal herniation is known as transtentorial herniation. 04:32 What is that going to do? It's going to press upon the brain stem. 04:36 Third cranial nerve, oculomotor. 04:39 What happens? You lose your parasympathetic, you have uninhibited sympathetic activity, blown pupil. 04:45 Uncal herniation also compresses the 6th cranial nerve, so the patient cannot move the eye outward. 04:51 Or you can have tonsillar. 04:52 What does that mean to you? What tonsils am I referring to? Cerebellar tonsils. 04:58 And these may herniate into where? The foramen magnum. 05:04 Topic: Increased intracranial pressure. 05:06 But at the same time, remember, there are many pathologies that could occur at the same time, giving you different, different, different presentations. 05:13 You just have to be very careful as to what exactly is the clinical picture. 05:19 So then you can choose the appropriate step of management.
About the Lecture
The lecture Increased Intracranial Pressure: Introduction by Carlo Raj, MD is from the course Increased Intracranial Pressure (ICP).
Included Quiz Questions
Which type of brain herniation may result in lower extremity symptoms?
- Subfalcine herniation
- Right uncal herniation
- Left uncal herniation
- Cerebellar tonsillar herniation
- Right transtentorial herniation
Which type of abnormality is seen with a transtentorial herniation?
- Compression of the brainstem
- Communicating hydrocephalus
- Compression of the cingulate gyrus
- Compression of the parietal lobe
- Compression of the thalamus
What is the primary cause of brain herniation?
- Increased intracranial pressure displacing the brain into the foramen magnum
- Increased intracranial pressure causing pressure on the spinal cord
- Decreased intracranial pressure causing increased cerebral perfusion pressure
- Encephalitis
- Birth defects
Author of lecture Increased Intracranial Pressure: Introduction

Carlo Raj, MD
Customer reviews
3,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
2 |
| 1 Star |
|
1 |
exactly what needs to be understood about intracranial pressure. clear and easily understood
Lecture was excellent! very clear and simple. I enjoyed it. Thanks so much Dr Raj.
Some of Dr Raj's lectures are excellent, but this is one of the frequent examples of his strange mannerisms obstructing a clear explanation.
Provided no useful explanations on the topic and I ended up looking for information on google to understand it myself. To much joking around and too little professionalism.
