Playlist
Show Playlist
Hide Playlist
Other Types of Pneumonia


-
Slides 01 URTIBronchitisPneumonia RespiratoryAdvanced.pdf
-
Download Lecture Overview
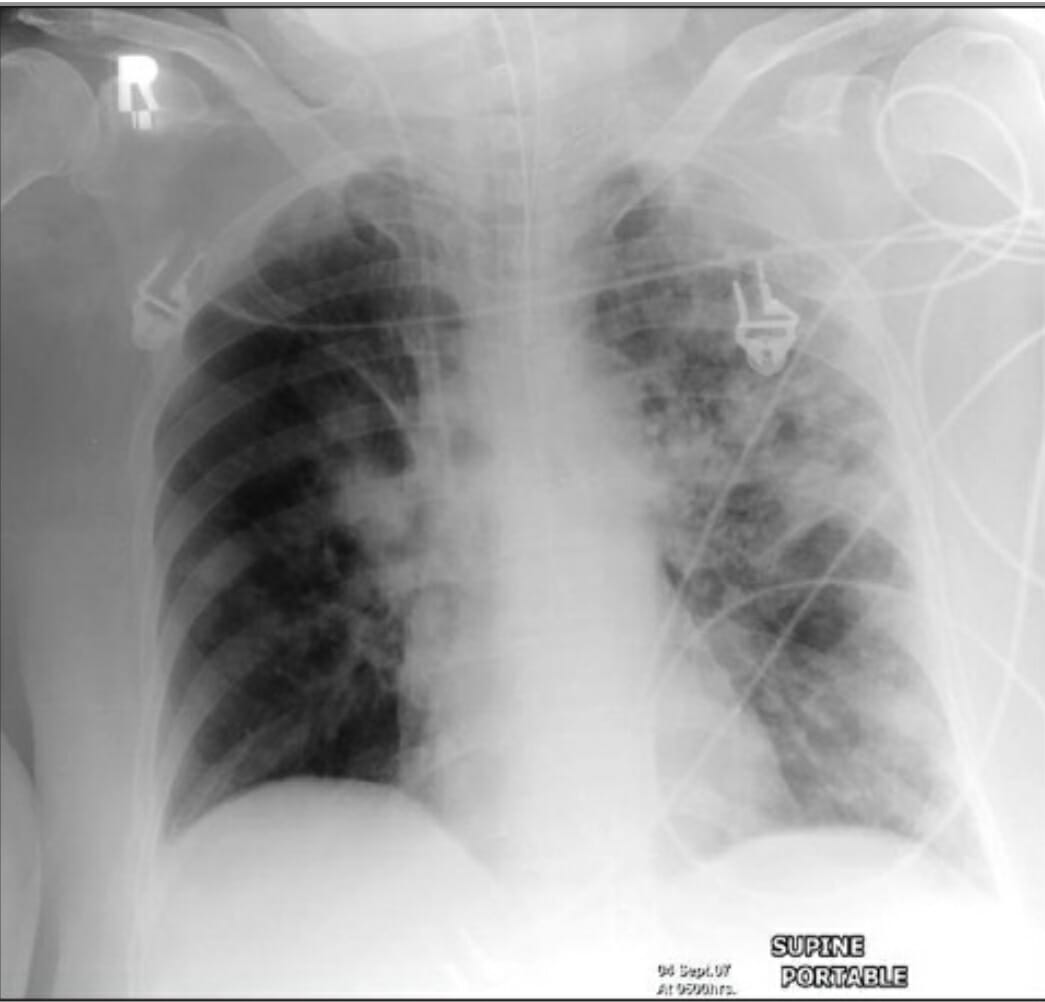
00:00 Right, so that's the discussion about community acquired pneumonia which is commonest form of pneumonia, and the one that most people will be dealing with most of the time. 00:10 There are, as I've mentioned earlier, other types of pneumonia, the hospital acquired, the ventilator acquired, and there is the immunosuppressed pneumonia. And the reason why we define these as separate to community acquired pneumonia is that the infecting organisms are going to be different. The chance of having a standard normal community acquired organism is much lower in hospital acquired disease. So for example hospital acquired pneumonia, the common organism causing disease in those circumstances will be Staphylococcus aureus, and the gram-negative bacteria: Klebsiella, E. coli Serratia and Pseudomonas aeruginosa, and these organisms are harder to treat, and do not respond to the standard amoxicillin and macrolide therapy that you use for community acquired pneumonia. So they require very specific treatments. Immunosuppressed patients, because of that effects of having a very weak immune system, suddenly the patient is actually exposed to infection with a whole range of microorganisms that don't normally affect people, and that doesn't just include bacteria. The bacteria will be the same as you might get it in a hospital acquired disease, but in addition there are a range of viruses, cytomegalovirusese which may cause infection in these circumstances, and cause severe disease. And in addition, the respiratory viruses that in most people are self-limiting and very mild disease parainfluenza, adenovirus, etc. rhinovirus, cause much more severe disease in the immunosuppressed patient. 01:36 And in addition, there is a range of organisms, fungi which you may get infected with in the immunosuppressed which would never normally infect somebody who's got a normal immune system, and that's mainly Aspergillus and Pneumocystis jirovecii. So hospital acquired pneumonia is important because actually it is the commonest fatal hospital acquired infection. So you need to know about this, as a disease that requires close attention and aggressive treatment when it develops. For treatment it needs to cover the organisms as we discussed, Staphylococcus aureus, the gram-negatives, and pseudomonas. 02:13 Empiric treatment with broad spectrum I.V. antibiotics is started while waiting for the results of the sputum in blood cultures to guide specific therapy. 02:21 Things to consider include recent antibiotic therapy, comorbidities and likelihood of multiple Drug-Resistant or MDR pathogens. 02:30 This can be seen in the hospital antibiogram. 02:32 The initial antibiotic therapy depends on several factors. First, if there's a low risk for multiple Drug-Resistant pathogens, piperacillin/tazobactam or cefepime can be used. 02:44 If there's a higher risk for multiple drug resistant Pseudomonas amikacin can be added to the regimen. 02:49 And finally, if there's a risk for resistant Pseudomonas and MRSA, you can add vancomycin or linezolid to the regimen. 02:57 Remember, the dosing needs to be adjusted based on the patient's renal function. 03:01 The actual presentation of hospital acquired pneumonia is pretty much the same as community acquired pneumonia, cough, fever, shortness of breath, and with new consolidation, a rise in the markers of inflammation. Pneumonia in immunocompromised is very much more complex than normal pneumonia because of this extended range of organisms that may be causing the problems. And again, just to reiterate we are talking about patients who have really quite marked immunosuppression. They have had to have a organ or bone marrow transplantation. They’ve been receiving chemotherapy or high-dose cytotoxic agents or biological agents to immunosuppress them because of a major inflammatory disease such as connective tissue disease, or they have HIV infection with a low CD4 count, or they have a hematological malignancy which by their very nature affect the white cells and therefore make you much more immunosuppressed that you would be normally. The situation here is that there is such a large range of organisms, the decision about treatment options is much more complex than it would be in a normal person presented with a community acquired pneumonia, because you may need to treat respiratory viruses, you may need to treat cytomegalovirus, you need to treat for the organisms that make hospital acquired pneumonia, and then there are the fungi, Aspergillus and Pneumocystis, and unfortunately, Aspergillus and Pneumocystis require very different treatments. So it is a very complex situation that requires clinical assessment to make sure the right medication is given to the patient, and often these patients will end up on antibacterials, antivirals, and antifungal agents, because we are not quite sure what's going on. This is a CT scan showing what an invasive fungal infection looks like after a stem cell transplant with focal disease at the top of the right lung.
About the Lecture
The lecture Other Types of Pneumonia by Jeremy Brown, PhD, MRCP(UK), MBBS is from the course Infections of the Respiratory Tract.
Included Quiz Questions
Which of the following is an example of a severely immunocompromised patient in which pneumonia may develop?
- Patients receiving chemotherapy
- Patients planning to undergo bone marrow transplantation
- Patients who have a history of tinnitus
- Patients with active HIV infections and high CD4 count
- Patients diagnosed with inflammatory bowel disease
Which of the following is the most commonly fatal hospital-acquired infection?
- Hospital-acquired pneumonia
- Central line-associated blood stream infection
- Catheter-associated urinary tract infection
- Surgical site infection
- Urinary tract infection
Which of the following is an appropriate choice of antibiotics in a patient with ventilator-associated pneumonia?
- Amoxicillin/clavulanic acid + ciprofloxacin + ceftazidime
- Amoxicillin/clavulanic acid
- Amoxicillin
- Amoxicillin/clavulanic acid + clarithromycin
- Amoxicillin + clarithromycin
Which of the following statements is FALSE regarding pneumonia in immunocompromised patients?
- The presentation of pneumonia in immunocompromised hosts is identical to that of pneumonia in healthy individuals.
- Pneumonia in immunocompromised hosts is caused by a larger range of organisms.
- Treatment of pneumonia in immunocompromised hosts is complex.
- Most immunocompromised patients with pneumonia are treated with antibiotics, antivirals, and antifungal agents.
- Pneumonia in immunocompromised hosts can be caused by atypical organisms like Pneumocystis jirovecii.
Which of the following statements is FALSE regarding hospital-acquired lung infections?
- Hospital-acquired pneumonia is treated with narrow spectrum antibiotics.
- Hospital-acquired pneumonia can present similarly to community-acquired pneumonia.
- Ventilator-associated pneumonia is pneumonia acquired while intubated and ventilated.
- Hospital-acquired pneumonia may arise from a broader spectrum of microorganisms.
- Hospital-acquired pneumonia is the most commonly fatal hospital-acquired infection.
Author of lecture Other Types of Pneumonia

Jeremy Brown, PhD, MRCP(UK), MBBS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
