Playlist
Show Playlist
Hide Playlist
Hirschsprung Disease

-
Slides GIP Hirschsprung Disease.pdf
-
Download Lecture Overview
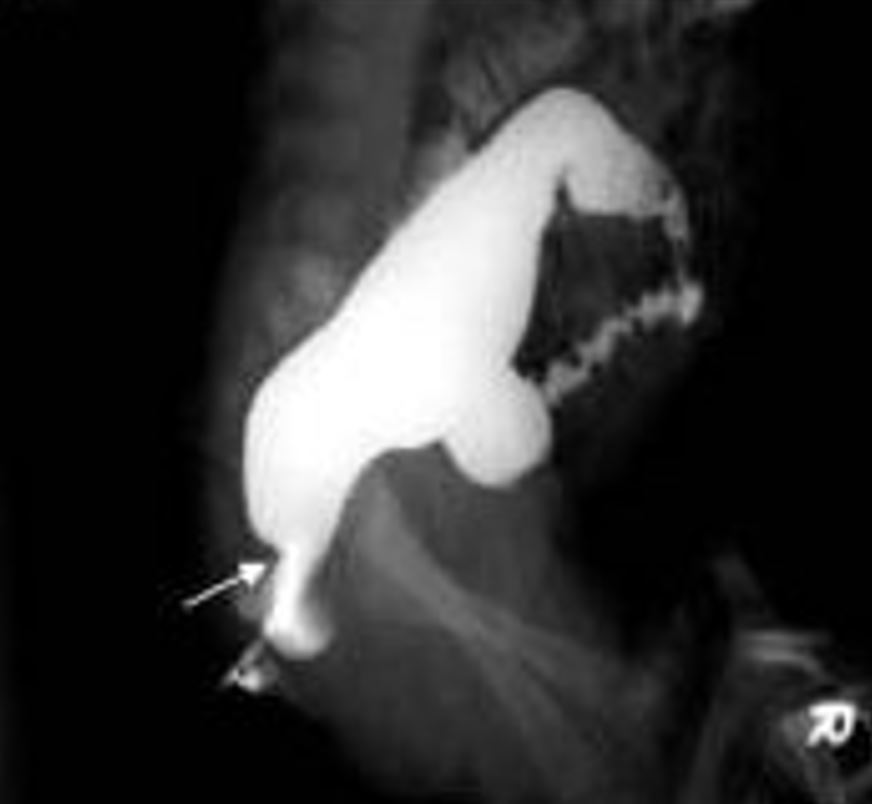
00:01 Welcome. 00:02 This talk is all about Hirschsprung disease. 00:05 You may not have heard about this before but now you will. 00:09 Hirschsprung disease is also called congenital megacolon. 00:13 And basically it's caused by the failure of neural crest derived ganglion cells to migrate all the way along the length of the colon down to the anus. 00:25 The epidemiology, this is kind of interesting, about 1 in 5,000 live births in the US and that same frequency happens pretty much around the world. 00:35 It is much more common entity in baby boys than in baby girls. 00:40 There may be a more, a greater predilection in certain populations of Asian descent. 00:48 The pathophysiology involves mutations in the RET tyrosine kinase. 00:55 So, in these genes, that would normally control the growth and differentiation of neural crest cells there's a loss of function in these genes. 01:04 Most commonly, it is the RET gene. 01:07 So RET stands for rearranged during transfection gene and as a receptor tyrosine kinase loss of function of the RET tyrosine kinase in the neurons leads to the Hirschsprung disease. 01:22 Interestingly, there are other diseases associated with gain of function so constitutive activation of the RET tyrosine kinase. 01:30 That gain of function mutation in other tissues associated with various cancers including the multiple endocrine neoplasias, types lla and llb. 01:42 Interestingly, RET mutations, the loss of function mutations associated with Hirschsprung disease may also be influenced by environmental factors, some of which may be sex linked, and those can then modify the severity of the final disease. 02:03 In Sporadic Hirschsprung's disease, which is most common, about 70% of cases, a third of those may have RET mutations. 02:13 There are other mutations and that may lead to similar loss of normal migration of the neurons. 02:21 In familial disease, approximately half of the cases will have RET mutations. 02:25 And again, there are other known signaling molecules that may be involved in the normal migration of these neurons. 02:34 When it's part of the genetic syndrome, the RET mutations or other mutations are frequently associated with Down syndrome or Trisomy 21. 02:45 The Waardenburg syndrome which is associated with abnormal melanocyte migration and melanocytes are neural crest-derived cells. 02:53 So, it makes kind of sense that defects in melanocyte migration might also be associated with defects in the neural migration in Hirschsprung disease. 03:05 Additional congenital malformations are present in about a quarter of individuals, again, speaking to syndromic genetic changes. 03:14 And frequently there is congenital heart disease. 03:17 And in fact, in those who have Down syndrome, trisomy 21, there's a very high prevalence of cardiac heart anomalies. 03:29 So normal peristaltic movement within the GI tract. 03:33 This is normal movement squeezes the bowel contents from proximal-to-distal. 03:37 This top-to-bottom trajectory requires the coordinated activity of parasympathetic ganglia and nerve plexi that sit within the layers of the muscularis propria. 03:47 So the major layers of smooth muscle around the bowel, and in particular, we're going to be talking about Auerbach Myenteric Plexus. 03:55 During development, the nerves responsible for this activity must migrate from the original location in the neural crest, and traffic all the way along the elongating bowel eventually reaching completely to the rectum. 04:09 In Hirschsprung's disease, mutations and again, chiefly in the RET tyrosine kinase gene cause the cells to lose their ability to have the normal cellular proliferation and movement and you have an incomplete migration. 04:23 Sometimes, fortunately, this only involves just the very last bit of the rectum at the most distal end of the migratory path. 04:31 But sometimes it can affect the entire large bowel and even parts of the small bowel. 04:36 In most cases, the migration of the neurons ends somewhere in the sigmoid colon in patients who are going to have Hirschsprung disease. 04:44 When this happens, the affected portions of bowel are no longer able to transmit a peristaltic wave and they tend to just kind of sit there in a hyper contracted state, so they don't relax and they don't move the peristaltic wave. 04:57 That hyper contracted state of that portion of the bowel interferes with the passage of stool contents. 05:03 Depending on how much of the bowel is affected, therapy can range from just dilating the rectum to complete surgical resection of the affected portion of the bowel. 05:13 Gross pathology is pretty obvious when you think about what's going on at the molecular and cellular level. 05:20 So there is muscular hypertrophy and dilation of the bowel proximal to the obstruction. 05:24 Clearly, the bowel is trying to squeeze past the area of obstruction. 05:30 With that hypertrophy, and then dilation due to the obstruction, you may progress to a megacolon, and even rupture, which typically would occur in the cecum. 05:40 In Hirschsprung disease, the rectum is always involved, that's the most distal end of the migratory pathway. 05:46 In short-segment disease, you'll have involvement of the rectosigmoid colon, and that's going to be the most common manifestation. 05:54 And if we have extension more proximal to the sigmoid, so called long sigmoid disease that occurs in about 15% to 20% of patients. 06:03 It's relatively rare to have total colonic aganglionosis, and that's only 5% of cases or less. 06:12 So what's being demonstrated on the right in the histology, on the top is the normal layers of smooth muscle, we have an inner circular layer of the muscularis propria. 06:24 And we have an outer longitudinal layer of the muscularis propria, and in between are ganglia of the Auerbach's Plexus, that's going to be responsible for coordinating their movement. 06:35 In the bottom slide, on the right hand side, So this portion of the bowel is not innervated and can't undergo peristalsis. 06:46 And so now we're going to have that hyper contracted bit of smooth muscle in that location. 06:51 This is what's been shown on the left. 06:53 So all the way down on the kind of the bottom on the right, we have the Rectosigmoid which is a little shriveled kind of worm-like structure that has never been able to have a normal peristaltic wave. 07:07 That hyper contraction of the smooth muscle in that location due to the loss of the ganglia is going to cause more proximal bowel dilation. 07:17 And you can see that massively dilated segment all the way over into the small bowel on the left hand side. 07:25 The clinical presentation. 07:27 There's a classic triad, so babies don't pass meconium. 07:31 That's the early bowel contents of within the typical two days after birth. 07:38 Because there is now this proximal dilation due to the distal stenosis, you will have expanded abdominal contents and abdominal distension. 07:49 And because the baby is not able to move, bile, and anything that's ingested more distally, it tends to eject with forceful bilious vomiting. 08:00 Additional signs and symptoms. 08:01 So depending on the degree of obstruction, if there's just a little bit at the very distal rectum, you can actually do a digital rectal exam and allow massive release of air so there'll be an explosive expulsion of gas and stool. 08:21 Depending on inflammation that may be associated with the dilation depending on ischemia, you may have an enterocolitis. 08:30 And typically, if there's going to be a perforation, it's going to be at the level of the appendix or cecum. 08:37 So how do we make the diagnosis? Not too hard. 08:41 So if we don't have the normal passage of meconium, we have distension of the abdomen. 08:46 If we have bilious vomiting, we're kind of suspicious that there may be obstruction someplace. 08:51 If we do a contrast enema, the lumen of the bowel is there, we just can't get stool to go through it because there is no relaxation. 09:01 It's a hyper contracted bit of smooth muscle in that portion of the bowel. 09:06 So if we do a contrast enema, going from below up, we will see a stenotic segment into dilated loops of bowel which is what you're seeing on the right hand side. 09:18 You can also do anorectal manometry. 09:20 So just put a pressure sensor up and see that there's a hyper contracted segment. 09:25 We can confirm our diagnosis by doing a rectal biopsy, a rather deep rectal biopsy into the muscularis propria. 09:33 And we can demonstrate there the absence of ganglion cells which will confirm the diagnosis. 09:39 In most cases, although I would always advocate for biopsy being a pathologist, we won't do this. 09:46 Managing the disease. 09:48 So, one, the most important thing is to recognize that it's there. 09:53 Once you have identified it, we also want to make sure because there are many syndromic manifestations. 09:59 Associated with Hirschsprung disease, you want to be sure there's nothing else wrong with the baby. 10:04 So we'll do a genitourinary ultrasound to assess for urinary system malformations. 10:08 We'll screen for hearing impairment, we'll screen for visual impairment. 10:13 We should also be looking to see whether there are any cardiac anomalies. 10:16 Remember that cardiac malformations are going to be commonly associated. 10:21 We should definitely get a clinical geneticist involved. 10:24 In cases where there may be mutations that would lead to multiple endocrine neoplasia types lla or llb. 10:33 Clearly, if there's a long segment of bowel, we can't just dilate it, we're going to have to surgically resected. 10:38 So we'll do a primary anastomosis from the normal functioning portion of the colon into the anus. 10:46 If there's really ultra short segment Hirschsprung disease, so just the last 3-4 cm from the internal anal sphincter, we can manage this with diet, stool softeners, laxatives, even botulinum toxin injections to cause a relaxation of the smooth muscle. 11:06 But in many cases, even that short segment will require some degree of surgical management with myomectomy cutting incising the smooth muscle so that we can get passage of stool. 11:19 With that, we've kind of covered all the way down to the very end of the colon with Hirschsprung disease.
About the Lecture
The lecture Hirschsprung Disease by Richard Mitchell, MD, PhD is from the course Small and Large Intestines Disorders.
Included Quiz Questions
What causes Hirschsprung disease?
- Failure of neural crest-derived ganglion cells to migrate into the distal colon
- Failure of neural crest-derived ganglion cells to migrate into the proximal colon
- Failure of neural crest-derived ganglion cells to migrate into the stomach
- Failure of mesenchymal ganglion cells to migrate into the stomach
- Failure of mesenchymal ganglion cells to migrate into the distal colon
Which gene is associated with Hirschsprung disease?
- RET
- EGFR
- HER2
- BRCA1
- BRCA2
Which symptom is included in the triad of symptoms for Hirschsprung disease?
- Delayed passage of meconium
- Hypotonia
- Non-bilious vomiting
- Vomiting
- Bleeding
What is NOT a common symptom of Hirschsprung disease?
- Projectile vomiting
- Abdominal distension
- Bilious vomiting
- Explosive stool
- Enterocolitis
What will a contrast enema show in Hirschsprung disease?
- Distal stenosis of the bowel
- Triple bubble sign
- Double bubble sign
- Bird's beak sign
- Circumferential margin obliteration
Author of lecture Hirschsprung Disease

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
