Playlist
Show Playlist
Hide Playlist
Chronic Kidney Disease (CKD): Definition with Case

-
Slides Nephrology Chronic Kidney Disease.pdf
-
Download Lecture Overview
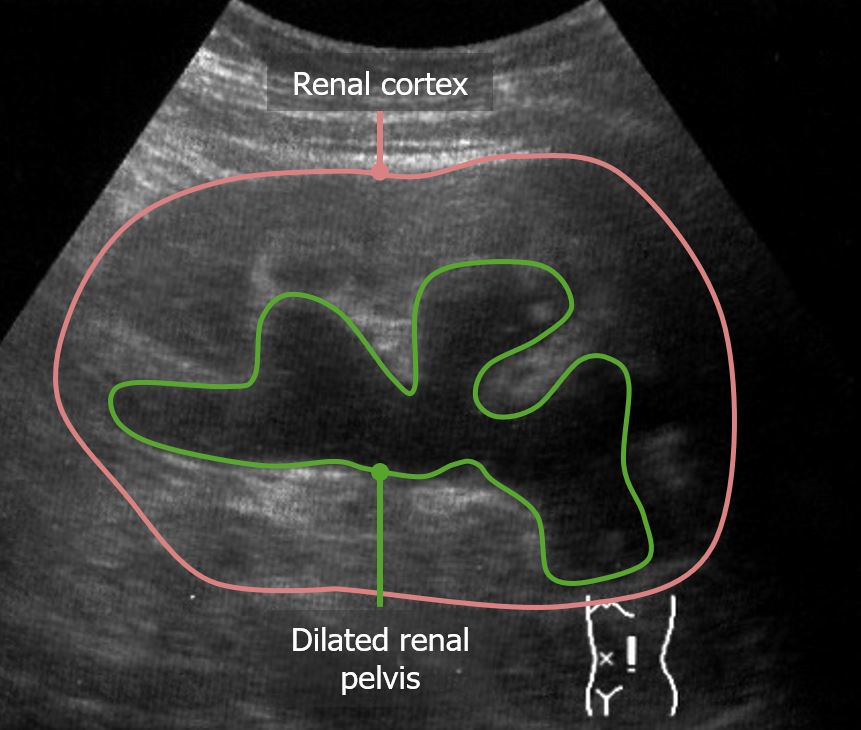
00:01 Hello and welcome to the Nephrology curriculum. 00:04 Today we're going to be talking about chronic kidney disease. 00:07 And if you're taking care of patients, you will definitely encounter patients who have chronic kidney disease. 00:11 So it's important to understand it. 00:15 Let's start out with a clinical case. 00:17 A 29 year old woman, is noted to have microscopic hematuria with two plus positive-dipstick proteinuria. 00:24 And remember, of course no proteinuria on the dipstick is normal. 00:28 And this is taken on screening labs for a life insurance policy. 00:32 It was confirmed on a repeat urine analysis three months later at her primary care doctors office. 00:37 Her serum creatinine however as normal. 00:41 Now let's go to another case of a 52-year old man with a history of hypertension who is noted to have a serum creatinine at 1.7 milligrams per deciliter and we can see by the normal values that that's elevated. 00:53 His urine analysis however is unremarkable. 00:56 In review of his past records, His serum creatinine was also elevated to 1.7 milligrams per deciliter about six months prior. 01:04 So the question is which one of these patients has chronic kidney disease. 01:10 Let's go through the history and see if we have some clues to our diagnosis. 01:14 So in our first case of a woman who's going for her life insurance policy, she has a history of microscopic hematuria and proteinuria and it sustained over time because when she reject her Labs at three months time, she also had hematuria. 01:29 So that's really suggestive of chronic kidney disease in terms of that there's clinical damage to the kidney. 01:36 How about our second case of our gentleman who has an elevated creatinine. 01:40 A high creatinine means that his GFR or glomerular filtration rate is lower. 01:45 And again, this has been sustained over a three-month period of time. 01:49 So this gentleman has chronic kidney disease as well. 01:53 So the answer is that they both actually have chronic kidney disease. 01:58 So how exactly do we define chronic kidney disease? It's really based on either having kidney damage or decrease in GFR over time. 02:06 Let's focus a little bit more closely on kidney damage. 02:09 What does that mean exactly? It could be that there's a pathologic abnormality of the kidney meaning that if my patient perhaps is diagnosed with IGA nephropathy. 02:18 I have a renal biopsy. 02:19 I look at that biopsy and I see evidence of clinical disease with IGA nephropathy. 02:24 Even though their creatinine is normal. 02:26 Let's say it's 0.7. 02:28 They still have evidence of disease by biopsy. 02:32 It could be clinical markers of kidney damage. 02:34 That would be something like proteinuria. 02:36 So normally we excrete less than a hundred fifty milligrams of protein in her urine when it exceeds that greater than a hundred fifty milligrams and that sustained over time, that would also be a marker of having kidney damage. 02:50 Albumin which is which is the principal component of protein in the urine if that is greater than 30 milligrams that also exceeds the threshold of having normal values so that patient will also have evidence of clinical damage if that sustained over time. 03:06 Glomerular hematuria is another sign of clinical damage. 03:10 That means that you have those funny shaped red blood cells, we call them dysmorphic because they have funny shapes on their membrane as they have bloods, blebs since they transverse that glomerular basement membrane. 03:21 We can also see things like red blood cell casts when we see that clinically, we know that that patient likely has glomerular damage. 03:31 Other clinical markers of kidney damage include Imaging so I might have a patient who has polycystic kidney disease and they potentially could be early in their course. 03:40 So again could have a normal serum creatinine, but when I image them with something like an ultrasound I might see multiple cysts which would indicate that that patient also has chronic kidney disease. 03:51 I might be seeing something like hydronephrosis on ultrasound. 03:55 So this is an ultrasound that shows a kidney that has hydronephrosis essentially that's urine that's backing up into that renal pelvis So you see that big dilated renal pelvis that big boggy cortex if that sustained over time that is also a clinical marker of kidney damage, and finally, here's an ultrasound that shows a kidney that's very echogenic meaning that it's brighter than the liver on ultrasound and you can see that the cortex is quite thin. 04:21 When that happens, that's also a marker of chronic kidney disease despite the fact that the serum creatinine might be normal. 04:27 So it's important to keep that in mind. 04:30 Now we also talked about another way to mark kidney damage is a decrease in kidney function that would also signify that that patient has chronic kidney disease, and I think that's what most of us traditionally think about when we have a patient with chronic kidney disease. 04:45 That means that the GFR or glomerular filtration rate is less than 60 mils per minute per body surface area for greater than 3 months duration. 04:56 So just keeping in mind a normal GFR for most people is somewhere between 90 and 120 mils per minute. 05:04 Now this decrease in GFR of less than 60 mils per minute really needs to be sustained over time meaning that we have to have at least two measurements separated at least two weeks in addition to that greater than 3 months of decrement and function. 05:18 We want to make sure that that's real.
About the Lecture
The lecture Chronic Kidney Disease (CKD): Definition with Case by Amy Sussman, MD is from the course Chronic Kidney Disease (CKD).
Included Quiz Questions
Which of the following is required for a diagnosis of chronic kidney disease (CKD)?
- Persistent evidence of kidney damage or a decrease in function for at least 3 months
- Hematuria with dysmorphic red blood cells
- Heavy proteinuria (protein excretion greater than 3.5 g/24 hours)
- Oliguria (urine production less than 0.5 mL/kg/day)
- Multiple cysts on renal imaging
Which of the following is considered a clinical marker of kidney damage?
- Albuminuria
- Hyaline casts on urinalysis
- Decreased blood urea nitrogen
- Decreased creatinine
- Bilirubinuria
Which of the following statements is true regarding chronic kidney disease (CKD)?
- An echogenic kidney with thin cortices on ultrasonography is a marker of CKD.
- A low glomerular filtration rate is a requirement to diagnose CKD.
- A single abnormal glomerular filtration rate measurement is sufficient to diagnose CKD.
- A renal biopsy is necessary to diagnose CKD.
Author of lecture Chronic Kidney Disease (CKD): Definition with Case

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
