Playlist
Show Playlist
Hide Playlist
Acromegaly

-
Slides 01-02-01 Adrenal Pituitary.pdf
-
Download Lecture Overview
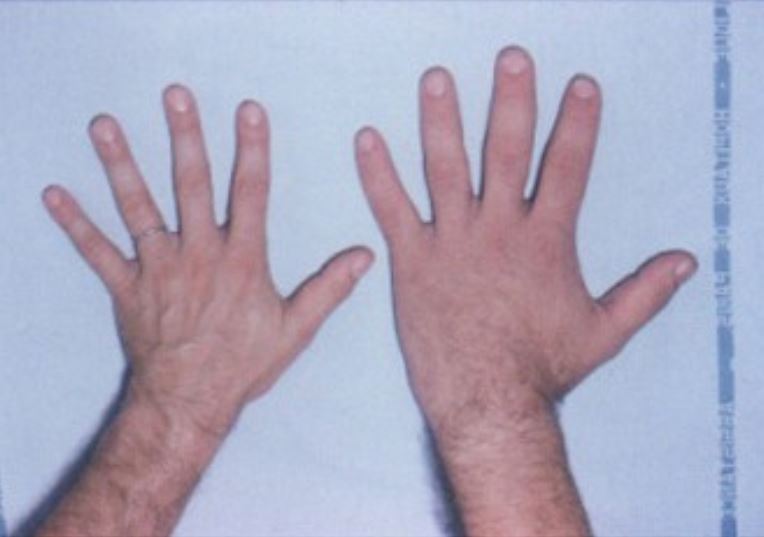
00:01 Growth hormone is pulsatile throughout the day and is not useful for the diagnosis of acromegaly. 00:06 The best screening test is a serum IGF-1 or insulin-derived growth factor. 00:13 Excess growth hormone is confirmed with an oral glucose tolerance test because glucose normally suppresses growth hormone levels to less than one nanogram per ml. 00:24 Growth hormone levels greater than one nanogram per ml are diagnostic of growth hormone excess. 00:31 Anterior pituitary MRI should be obtained once growth hormone excess is confirmed by chemically to rule out a pituitary lesion. 00:39 Acromegaly is the clinical syndrome that occurs when a pituitary tumor secretes excessive amounts of growth hormone in an adult patient. 00:48 Prior to puberty, patients with growth hormone-secreting tumors develop excessive longitudinal growth and gigantism above normal for age. 00:59 Let's go through some of the external features of acromegaly again. 01:03 In the head, there may be prominence of the brow and jawline. 01:06 There may have been an enlarged skull. 01:08 There may be facial edema and coarsening of facial features, excessive spacing between the teeth usually of the lower jaw, and finally, macroglossia or enlargement of the tongue. 01:20 The skin can demonstrate thickening and skin tags, and the hands and feet may be disproportionately large. 01:28 In the joints, arthritis may be a manifestation, and other internal features include diabetes mellitus, hypertension, colon polyps, and excessive perspiration or hyperhidrosis. 01:43 Obstructive sleep apnea is usually caused by excessive growth of tissue in the upper airway, and in and around the mouth, along with macroglossia, which leads to obstructive symptoms when sleeping. 01:57 Left ventricular hypertrophy can occur in the heart, and these patients may present with cardiomyopathies. 02:03 And then finally, there are increased rates of cancers, particularly of the colon, esophagus, and stomach, as well as thyroid, and even melanomas. 02:12 The clinical poll here is in clinical practice. 02:15 Because of the increased number of colonic polyps, patients are predisposed to colon cancers, and will often present, as a first feature, with blood in the stool. 02:26 The treatment of acromegaly requires transsphenoidal tumor resection, and surgery is the only treatment that is potentially curative. 02:35 Remission is achieved when IGF-1 levels are within the normal range for age, and the response of growth hormone to glucose tolerance test returns to normal. 02:44 Patients not achieving remission require injectable somatostatin analogues to inhibit growth hormone secretion. 02:52 High-dose dopamine agonist therapy is marginally effective when the tumor co-secretes prolactin. 02:59 Pegvisomant, a growth hormone receptor blocker, is then used to lower IGF-1 levels, but it works in the peripheral tissues as an antagonist to growth hormone, and does not decrease growth hormone production by the tumor.
About the Lecture
The lecture Acromegaly by Michael Lazarus, MD is from the course Pituitary and Hypothalamic Disorders.
Included Quiz Questions
Which of the following tests is used to establish a diagnosis of acromegaly?
- Oral glucose tolerance test (OGTT)
- Liver function tests (LFTs)
- Hemoglobin A1C (HbA1c)
- Thyroid function tests (TFTs)
- Complete blood count (CBC)
Which of the following medications for acromegaly is a growth hormone receptor antagonist?
- Pegvisomant
- Octreotide
- Pasiriotide
- Cabergoline
- Lanreotide
Which of the following conditions does NOT occur as a consequence of acromegaly?
- COPD
- Cardiomyopathy and left ventricular hypertrophy
- Obstructive sleep apnea
- Hypertension
- Diabetes mellitus
Author of lecture Acromegaly

Michael Lazarus, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
