Playlist
Show Playlist
Hide Playlist
Neisseria Meningitidis (Meningococcus): Signs & Symptoms

-
Slides Meningitis InfectiousDiseases.pdf
-
Download Lecture Overview
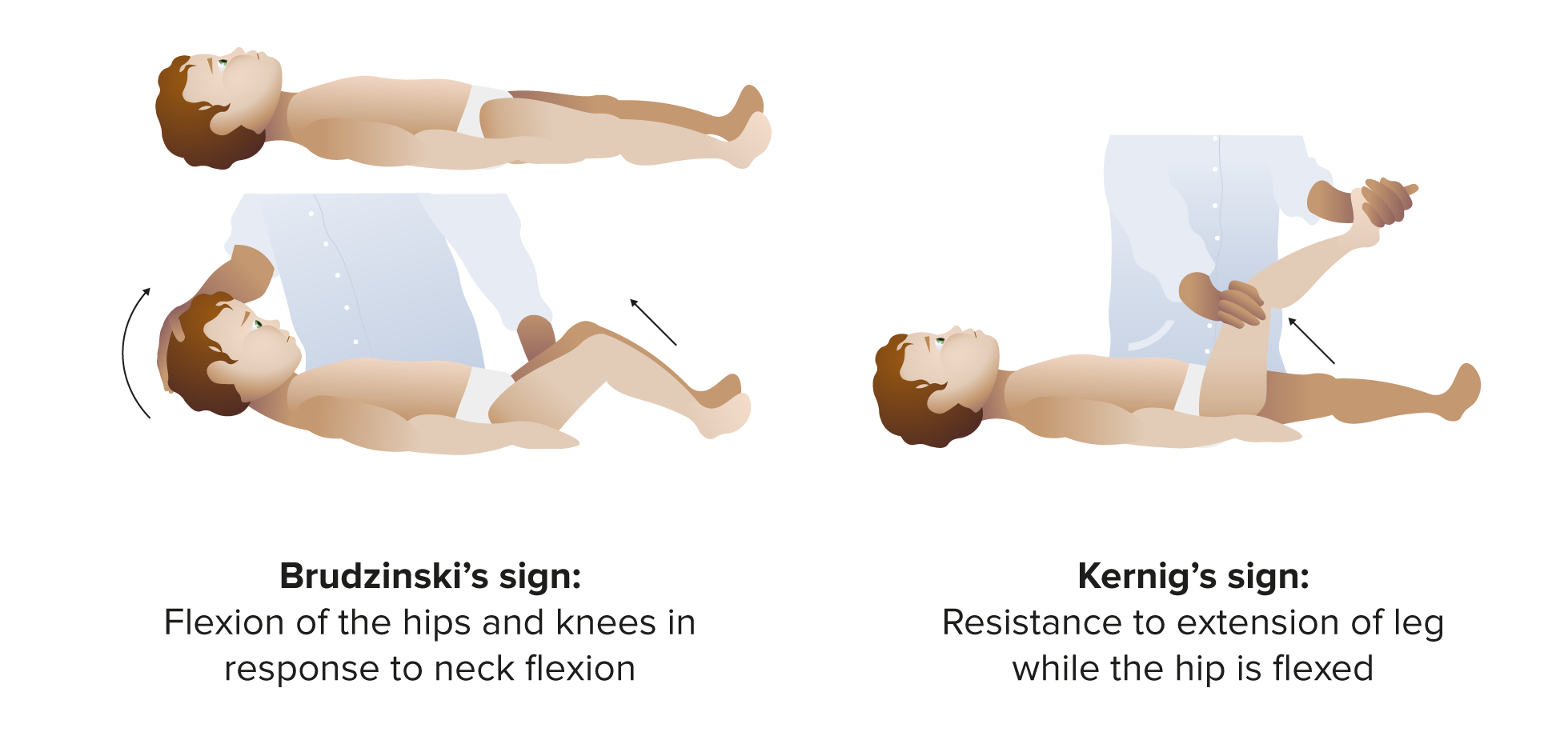
00:02 So, let's turn our attention to Neisseria meningitidis. 00:09 The incubation period is pretty abrupt and we’re usually going to find this in young adults or kids and it's especially common in college-age students, who live in a dormitory setting, or in military barracks - young people in military barracks. 00:30 And this is an abrupt illness. 00:33 These patients will have fever. 00:37 They will have a stiff neck. 00:41 Their blood pressure may be low. 00:44 And many of them, probably 50% of them, will have a rash, which I'll point out shortly. 00:53 And it's absolutely essential to make this diagnosis because the fatality rate is between 9% and 12%. 01:04 And up to 40% of the patients will have bacteria in the blood stream, so-called meningococcemia. 01:13 The other thing is, you can have meningococcemia without meningitis, but we’ll focus in this discussion on meningitis. 01:22 So, with meningococcemia - and you can have meningitis with it - you have fever and this petechial or purpuric rash. 01:34 And I want to just stop for a minute and tell you about a patient I saw years ago in my training. 01:43 A little girl was brought into the emergency room and she was a little bit lethargic and she had a little bit of low-grade fever, but otherwise was not that sick. 01:54 She did not have a stiff neck, for example. 01:59 But, anyway, because we were concerned about her lethargy, we decided that she needed to have a spinal tap. 02:07 So, we did a spinal tap while she was in the emergency room. 02:11 And in those days, we looked at the spinal fluid ourselves and we found that the spinal fluid was abnormal. 02:19 And we found all this out in about 30 minutes. 02:23 So, when we recognized that the spinal fluid was abnormal, we knew she had some form of meningitis. 02:30 So, in the emergency room, within 30 minutes of her arrival, we gave her intravenous penicillin because we were very concerned about her having meningitis. 02:43 And I'm sad to say that, four hours later, her skin was covered with the lesions that I'm showing you right here and she died. 02:55 And the main point about it is that meningococcal meningitis is one of the causes of sudden death. 03:04 So, it is essential to keep your antenna up for this particular illness. 03:12 The other thing about this rash is, if you were to put your finger down on some of these spots, they would not turn white under your finger. 03:25 You can also use a microscope slide and press down and you would find that these lesions do not go away with pressure. 03:36 So, the smallest ones are petechiae and the largest ones are really essentially bruises under the skin. 03:44 They’re ecchymosis. 03:47 And the point about this is this can develop over the course of hours. 03:51 It did in this little girl, despite giving her antibiotics. 03:57 The main thing in the differential diagnosis of this rash, there are other things that can do it. 04:03 I mentioned the pneumococcus, but there's one other thing, especially in the United States, and it's called Rocky Mountain spotted fever, which in itself has a 20% mortality. 04:15 So, the physicians, especially in the southeast, like in North Carolina, Virginia, Georgia, and those states in the southeastern United States where this is common, this disease, Rocky Mountain spotted fever, is actually spread by tick bite. 04:37 And it's different than meningococcemia initially. 04:42 Initially, the lesions of Rocky Mountain spotted fever will blanch when you press on them. 04:49 And over the course of several days, they can look like this rash of meningococcemia. 04:57 So, the pace with Rocky Mountain spotted fever is different. 05:01 But the bottom line is sometimes patients come in like this and you're not sure whether they have Rocky Mountain spotted fever or whether they have meningococcemia. 05:10 So, what you do is you treat for both. 05:12 You would treat both illnesses. 05:15 And Rocky Mountain spotted fever, the drug of choice is doxycycline. 05:21 I think that digression is important because these two diseases can really resemble each other. 05:28 Both of them can come along with hypotension and both can result in multiorgan failure. 05:37 In addition to the direct effects of meningococcemia, adrenal infarction leading to adrenal insufficiency can contribute to the hypotension and shock. 05:45 This is called the Waterhouse-Friderichsen syndrome. 05:48 So, turning to another cause of bacterial meningitis is that of group B Streptococcus. 05:55 And most of the people who get this, if their children have got it from some kind of middle ear disease, otitis media or perhaps mastoiditis, and for reasons that I'm not certain about, but diabetics seem to get an inordinate number of infections due to group B Streptococcus. 06:18 And this disorder carries with it fairly high mortality, at least in one series that I'm familiar with. 06:28 Listeria monocytogenes ordinarily looks like regular - like the other meningitidis. 06:37 But, occasionally, it can present as a granulomatous kind of meningitis and the spinal fluid can look different. 06:47 We’ll talk more about that later. 06:49 And then, very rarely, it can present as a rhombencephalitis. 06:55 In other words, presenting as inflammation of the back of the brain and the brainstem, with cranial nerve palsies, cerebellar signs, hemiparesis and altered consciousness. 07:08 So, this is a sneaky one, and so you need to know that it usually presents as a typical bacterial meningitis, but can rarely show other things. 07:19 Meningitis in the elderly is also a challenge. 07:26 It can present much more insidiously. 07:30 It can be sneaky. 07:31 Most of the elderly that have it are lethargic. 07:35 Most of them are out of it, but many elderly patients have Alzheimer's disease. 07:40 So, it's a challenge to figure out what's causing the altered mental status. 07:46 Occasionally, an elderly person will have no fever, and yet they will have meningitis. 07:54 Most of them have fever. 07:56 But if they don't have fever, that's a bad prognostic sign. 08:01 It's the most dramatic predictor of death on presentation. 08:05 If they have meningitis, but no fever with it, it suggests that the immune system is not very active. 08:14 They may or may not have signs of meningeal irritation, like a stiff neck or Kernig’s or Brudzinski sign. 08:22 And remember, a lot of elderly people have osteoarthritis of their cervical spine. 08:28 So, they have a stiff neck, even when they’re feeling well. 08:32 So, a stiff neck may be difficult to evaluate in an elderly person.
About the Lecture
The lecture Neisseria Meningitidis (Meningococcus): Signs & Symptoms by John Fisher, MD is from the course CNS Infection—Infectious Diseases. It contains the following chapters:
- Signs/Symptoms – Neisseria Meningitidis
- Streptococcus Agalactiae (Group B Streptococcus)
Included Quiz Questions
What is the typical incubation period for Neisseria meningitidis?
- 3 to 4 days
- Less than 1 day
- 2-4 weeks
- 12-16 days
- 1-2 months
A 19-year-old college student recently went hiking with his dormitory friends in the mountains of the southeastern part of America. He now presents to the emergency room with fever, malaise, and a full body non-blanching petechial rash. He is hypotensive and tachycardic. Lumbar puncture and blood cultures have been sent to the laboratory. Which of the following diseases are the most likely diagnoses to be considered?
- Meningococcal meningitis and Rocky Mountain spotted fever
- Meningococcemia and bacterial pneumonia
- Viral meningitis and bacterial meningitis
- Lyme disease and meningococcemia
- Lyme disease and Rocky Mountain spotted fever
What is the approximate case-fatality rate of meningococcus meningitis?
- 9-12%
- 20-30%
- 45-50%
- Less than 1%
- 2-5%
A 2-year-old child is brought to the emergency department for a one-day history of lethargy, poor feeding, and episodes of vomiting. He had been tugging on his left ear for the past several days. He appears ill. On physical examination, he has a fever and is mildly tachycardic. Inspection of the neck shows nuchal rigidity. In the left ear, there are signs of otitis media. He does not have any rash. A lumbar puncture appears abnormal on the initial review. Which of the following organisms is most likely to be found in the cerebrospinal fluid?
- Streptococcus agalactiae
- Listeria monocytogenes
- Neisseria meningitidis
- Klebsiella pneumoniae
A 72-year-old man is brought in from the nursing home for increased lethargy and altered mental status from his baseline. Caretakers note that he has not had any fevers, but hasn't been eating well and appears to be moving more slowly than usual and avoiding turning his head. He does not have any rash. Lumbar puncture confirms meningitis. Which of his symptoms is most predictive of mortality from this illness?
- Absence of fever
- Evidence of meningismus
- Altered mental status
- Absence of rash
- Decreased appetite
Author of lecture Neisseria Meningitidis (Meningococcus): Signs & Symptoms

John Fisher, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Clinical anecdotes are a great supplement to an already helpful lecture
His anecdotes are amazing here. Makes the subject much more memorable.
