Playlist
Show Playlist
Hide Playlist
Derivatives of the Intermediate Mesoderm: Kidneys and Suprarenal Glands

-
Slides 08-47 Derivatives of the Intermediate Mesoderm.pdf
-
Download Lecture Overview
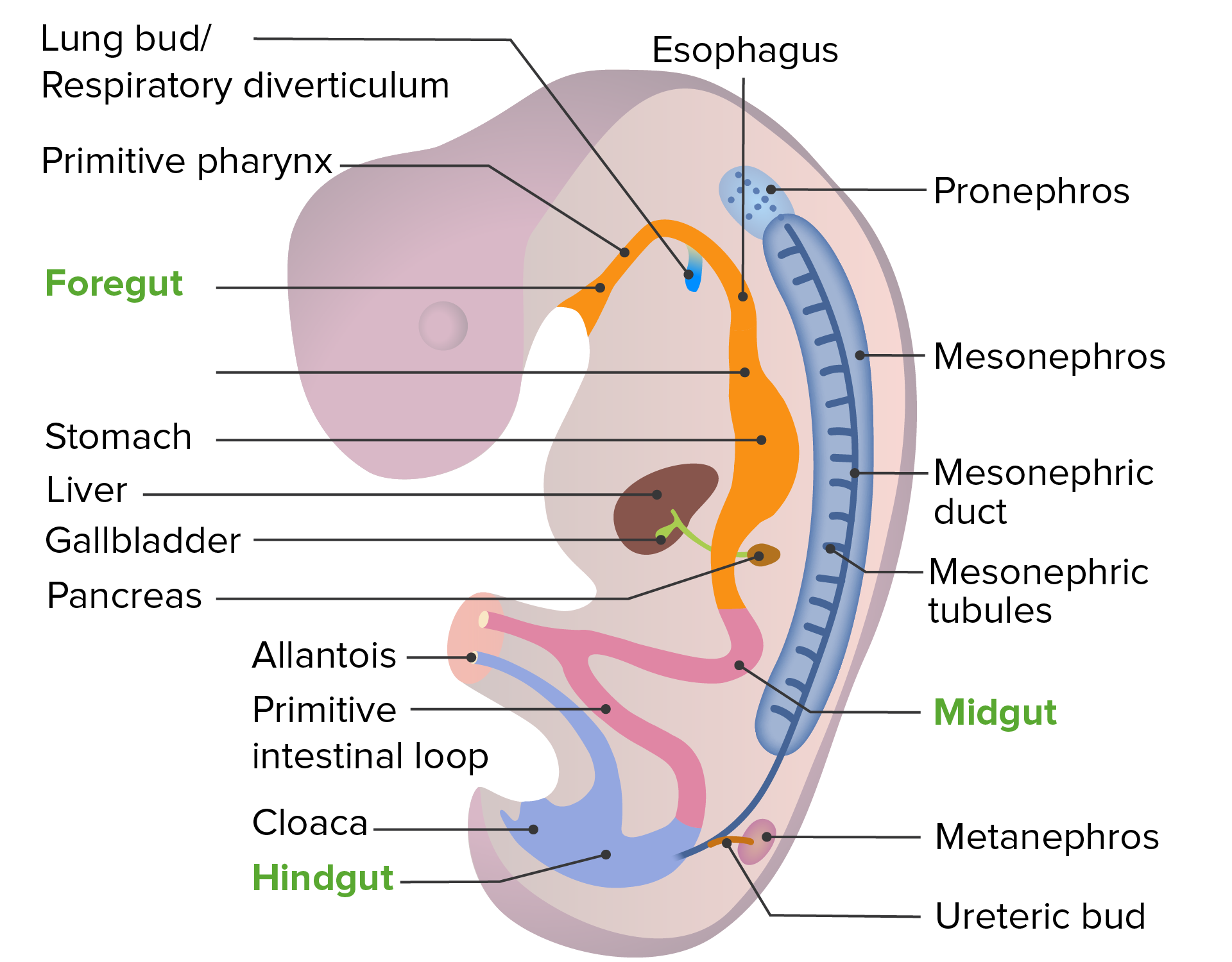
00:01 We will now begin discussing the development of the intermediate mesoderm and the structures that come from it. 00:07 We’re gonna start by discussing how the kidneys and suprarenal glands form. 00:11 Now, interestingly the renal and reproductive systems are both derived from the intermediate mesoderm and both are linked atomically and developmentally. 00:20 Now, without too much difficulty you can come up with a couple of connections between the reproductive and urinary systems. 00:26 In males, we have the reproductive glands and tracts emptying into the urethra along with the urinary bladder. 00:34 In females, we have a separate ureter and separate vaginal opening but they both empty into the vestibule, however, there are multiple developmental connections as well particularly that we have the intermediate mesoderm creating a succession of kidneys and some of those structures will seize to function as kidneys but contribute to the reproductive system so let’s start the process of examining that development right now. 00:58 We’re gonna return to my favorite slide the trilaminar embryo where organogenesis really, really, get started. 01:05 We’ve got the notochord on the midline, neurulation is beginning, got tube formation that’s gonna occur very soon and just beside the somites we have a little area colored kinda slightly yellowish orange that is the intermediate mesoderm and it is what’s going to create the kidneys and the gonads. 01:23 As the body will fold and the gut tube starts to form, we wind up with what’s referred to as the nephrogenic chords developing in the intermediate mesoderm. 01:34 Now, on the surface of those chords we’re gonna have urogenital ridges formed in contact with the developing body cavity. 01:41 The nephrogenic chords are the primordia of the kidneys and the urogenital ridges are the primordia of the gonads - the testes and the ovaries. 01:49 We’re gonna follow kidney development in this talk and return in a subsequent talk to the urogenital ridges. 01:56 So the nephrogenic chord forms not one, not two, but three sets of kidneys during development and only the third set becomes our actual adult kidney. 02:07 During weeks four to five, we have development of a structure called the pronephros in the embryonic cervical region and it forms but very quickly rescinds by the end of week five. 02:20 A little bit lower we have the mesonephros or middle kidney and it actually develops a mesonephric duct and it starts filtering urine, it actually does start filtering the blood stream but then regresses but the mesonephric duct remains and becomes an important structure in both the reproductive and urinary system. 02:43 And it’s important to the mature urinary system because of the very, very lowest portion of the mesonephric duct we get what’s called the ureteric bud, a little bleb of tissue moves off to the mesonephric duct and it’s going to induce formation of the final adult kidney and that is called the metanephros. 03:04 So we’ve gone from pronephors, to mesonephros, to metanephros and our adult kidneys actually start developing very far down in our pelvis and will ascend. 03:15 So here we can see that the metanephric kidney is shown at the bottom of the picture, it’s covered by the big kind of pinkly illustrated area there called the mesonephros. 03:27 So initially the metanephros and the ureteric bud are very close to the bladder but it will begin ascending as the mesonephros starts to degenerate and shrink and the gonads, ovaries, and testes come into existence. 03:42 Now as the metanephric kidney gets larger and more mature it actually starts ascending in the body. 03:50 Normally, ascent of this nature isn't caused by differential growth but as the kidneys move to more and more superior positions in the abdomen’s retroperitoneal region, they pick up a succession of arteries so they get the arteries from the iliac, vessels and then aorta and as they go further and further up they get more and more arteries and as they move old ones die off, new ones grow in. 04:15 As they move upward they’re going to encounter the suprarenal glands also known as the adrenal glands and I like to think of the adrenal glands sitting on top of these early metanephric kidneys like the hats on top of the guards, Buckingham Palace and they will form more superiorly whether or not the kidney is there so the adrenal glands are very close to kidney but you don’t need a kidney in order to have a suprarenal gland form and become functional. 04:43 Now because a succession of arteries are growing to supply the metanephric kidney it’s very common to have additional renal arteries having more than one renal artery is very common and in fact, you can have arteries coming into the superior or inferior pole of the kidney and those are just referred to as polar renal arteries. 05:05 Almost all the time, these additional arteries are clinically unimportant because they don’t cause any problems unless you are trying to remove the kidney or an inferior polar kidney obstructs drainage of the ureter which is trying to take the urine from the kidney to the urinary bladder. 05:22 So multiple renal veins are also frequently encountered and just have to be accounted for anytime a kidney is being removed and those vessels ligated. 05:30 Now, kidneys can fail to form - this is known as kidney agenesis and essentially a kidney will not form unless that ureteric bud comes off of the mesonephric duct so no ureteric bud, no kidney. 05:47 So kidney or renal agenesis can be problematic because you have half the number of kidneys but a single kidney can do the work that’s needed to keep the body healthy but it doesn’t have as much flexibility as you would if you had two kidneys as per normal. 06:04 As I mentioned before the suprarenal glands form completely separately, so your adrenal or suprarenal glands will be present on both sides even if there’s only one kidney. 06:14 Now, if we have failure of the ureteric bud to create a kidney, we can envision a few other problems that can occur such as if I have a ureteric bud that splits, I can wind up with what’s called a bifid ureter, a split ureter. 06:30 In this case a single ureteric bud went out from the mesonephric duct, split and induced the formation of a single kidney but it has two separate ureters and these can be relatively short or they could be relatively long. 06:45 This sometimes can happen if a ureteric bud grows out and splits widely and induces the formation of two kidneys it is possible to have three - one on one side, two on the other because of the splitting of the ureteric bud. 07:00 The illustration is also showing that occasionally the kidney may rotate to take the ureter and renal pelvis laterally although that’s fairly uncommon. 07:10 When you have a bifid split in the ureteric bud, you can induce the formation of two kidneys and occasionally you can induce two separate kidneys from two separate ureteric buds at which point you’re probably going to have two separate ureters draining all the way back to the urinary bladder so any variation on this theme is theoretically possible. 07:35 Other problems that can occur so the kidneys might form normally but fail to ascend. 07:40 These pelvic kidneys are not problematic in fact they usually work just fine and people may be unaware that they have it until an imaging study is done or a surgery is done in the area and the kidney is encountered, so these pelvic kidneys work just fine and in fact if surgeons have to transplant a kidney, it’s a great deal of trouble to try to stick a kidney into its normal place in the body and transplanted kidneys tend to be put into the pelvis in this pelvic kidney position because it’s easy to wire it into the bladder and easy to wire it into the blood supply nearby at the iliac arteries and veins. 08:18 A truly interesting thing happens if the two kidneys are in the pelvis and before ascending they fuse, these are called horseshoe kidneys and they are fused kidney made from two and they actually attempt to ascend but the problem is we've got the inferior mesenteric artery going to the hindgut and as that kidney ascends retroperitoneally, it’s going to wind up straddling that inferior mesenteric artery and it will be unable to go any higher and that straddling of the arteries would give it its horseshoe shape. 08:52 As with the pelvic kidney they don’t cause any problems they are functional and may only be encountered when imaging or exploratory surgery is being done. 09:01 Other problems involving kidney development are polycystic kidney disease. 09:09 Little cysts and occasional smaller cysts on kidneys are not actually that problematic. 09:15 Kidneys are very good at dealing with slightly reduce mass and you don’t get clinical signs of renal insufficiency until quite a bit of damage has been done but polycystic kidney disease causes a huge number of cysts to form on the kidney and generally, you're going to have to remove these because they keep enlarging bigger and bigger and you will have to have a kidney transplant done on the affected person sooner or later because these kidneys not only large but become non-functional. 09:44 There are two versions of it. Roughly, the autosomal dominant version happens when you have mutation of one of two genes, PKD1 or PKD2, which thankfully stand for polycystic kidney disease and they’re gonna lead to problems in calcium transport in the cilia of the kidney, that’s gonna result in inappropriate program cell death in the kidneys, apoptosis, causing a massive number of cyst to form. 10:11 There’s also another autosomal recessive version of it that comes from mutation of the PKHD1 gene but the same basic problem is encountered and it’s usually gonna be encountered during early infancy. 10:25 Okay. Thank you very much for your attention, I'll see you on our next talk.
About the Lecture
The lecture Derivatives of the Intermediate Mesoderm: Kidneys and Suprarenal Glands by Peter Ward, PhD is from the course Development of the Abdominopelvic Region. It contains the following chapters:
- Kidneys and Suprarenal Glands
- Developmental Defects of the Kidneys
- Polycystic Kidneys
Included Quiz Questions
Which of the following is false regarding renal and reproductive development?
- In development, the two systems are not linked.
- Both systems are formed from intermediate mesoderm.
- In development, both systems are linked anatomically.
- The nephrogenic cords are primordia of the kidney, but not the reproductive organs.
- The urogenital ridges are the primordia of the gonads, but not the kidneys.
Which of the following is false regarding the nephrogenic cords?
- They are primordia of the gonads.
- They form 3 sets of kidneys during development.
- They are the primordia of the kidneys.
- They are formed by intermediate mesoderm.
- The pronephros is the first kidney structure to form in development.
Which of the following statements regarding kidney precursors is TRUE?
- The final adult kidneys arise from the metanephros.
- Pronephros degenerates at the end of week 20.
- Metanephros forms in the cervical region.
- The connection between metanephros and the mesonephric duct becomes the urethra.
- Metanephric kidneys form in the pelvis and later descend further.
Which of the following is false regarding the movement of the kidneys during development?
- The suprarenal (adrenal) glands form atop the kidneys and move to the lower thoracic level as the kidney ascends.
- The metanephric kidneys form in the pelvis but ascend.
- Metanephric kidneys acquire a succession of renal arteries as they ascend.
- During ascent, the kidneys move to a retroperitoneal region.
- Additional renal vessels are relatively common as a result of the reception and loss of multiple arteries during development.
Which of the following is true regarding unilateral renal agenesis?
- It typically results from failure of the ureteric bud to form off the mesonephric duct.
- It typically results in oligohydramnios.
- It typically results in a horseshoe kidney.
- It typically results in a nonviable fetus.
- It typically affects the development of the suprarenal gland.
Which of the following is false regarding polycystic kidney disease?
- The autosomal dominant form typically causes poor kidney development during early infancy, resulting in very early clinical presentation.
- The autosomal dominant form can be due to a PKD-1 mutation.
- The autosomal dominant form can be due to a PKD-2 mutation.
- The autosomal recessive form is due to PKHD1 mutation.
- The PKD-1 and PDK-2 mutations lead to dysfunctional calcium transport in the cilia, resulting in apoptosis and cysts.
Author of lecture Derivatives of the Intermediate Mesoderm: Kidneys and Suprarenal Glands

Peter Ward, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Awesome teacher, really clear and easy to understand. The topic was nicely explained.
