Playlist
Show Playlist
Hide Playlist
Aortic Stenosis: Auscultation Areas

-
Slides ValvularHeart DiseaseAorticStenosis CardiovascularPathology.pdf
-
Download Lecture Overview
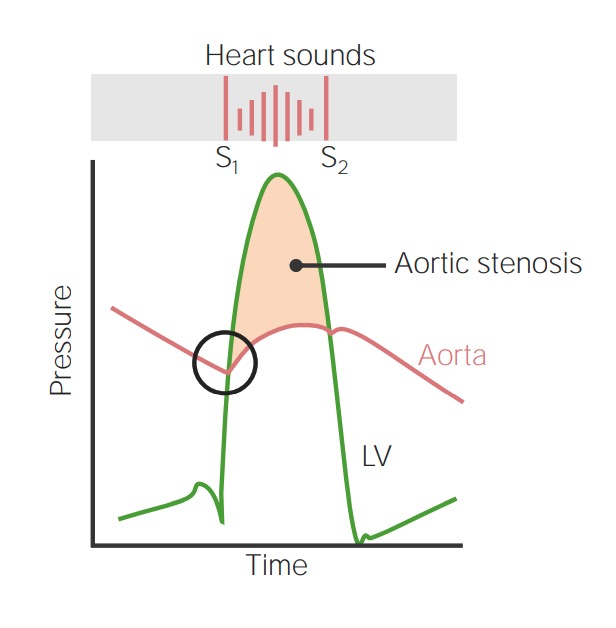
00:01 Valvular heart diseases. Where are we and what are we doing? My goodness. There is so much to discuss here, but approaches one valve at a time. And as we do so, we will dissect every single aspect of that valvular heart disease so that by the time you have gone through this, you know who your patient is, what they are presenting with and understand the pathogenesis of what guide is here in the first place. Let us begin. 00:29 Here once again is the chest. How important is this chest? Quite. We talked about the aortic area. I want you to point to it. Where am I? Right parasternal second intercostal space. Why? Because in anatomy of your aorta, take a look at the arch and so therefore, that is where you normally would hear your aortic valve. If you are dealing with a systolic murmur, take a look at aortic stenosis and I told you about that patient thus feeling tired, fatigue, maybe a little bit of chest pain with exertion. Let us talk about that for one second here. If it is aortic stenosis, what is causing this chest pain? It is not myocardial infarction, but it is the fact that with aortic stenosis, the left ventricle is having a hard time kicking against that increased afterload and so therefore the left ventricle is lifting weights. Once upon a time, when I was younger and I was lifting weights, I was undergoing hypertorphy of my biceps. Nowadays it is more about atrophy. 01:31 But as far as the left ventricle is concerned, it is also lifting weights. What are the weights in this environment? The stenotic aortic valve. So what is the hypertrophy that we were referring to in the left ventricle? It is the fact that it is concentric hypertrophy. Is that clear? And the reason I bring all this up is because with that increased thickness of the myocardium, that is a lot of myocardium in which blood has to continue supplying oxygen. So what if there was inadequate oxygention? Isn't that the definition of? Angina. Good. Let us continue. We also looked at the second intercostal space, left parasternal and that would be the pulmonic area. I want you to point it out. And here would be some type of pulmonic stenosis. 02:20 Here once again reiterate the atrial septal defect and why it would be a diastolic heart murmur that would be best heard by the fifth intercostal space left parasternal or best heard as a flow murmur through your second intercostal space, left parasternal because there is a lot of blood on your right side, right? Atrial septal defect. 02:44 Common causes, when we talked about ostium secundum and that would be congenital. But what if a child was born with unfortunately one of the most common causes of acquired intellectual disability in the United States is alcohol, acquired. So this is called fetal alcohol syndrome. It could be ASD? Sure it can. And with all of this blood moving from the left atrium to the right atrium, you have increased amount of blood and so the tricuspid valve now feels overwhelmed. And during your diastole, the tricuspid valve will open and with all this blood, which is pathologically being introduced into the right atrium is now moving forward, flowing in a turbulent nature into the right ventricle. Are you seeing this? And, therefore, atrial septal defect would be a diastolic murmur. Now at some point with all those blood, it would also hit the pulmonic valve. Clinically speaking you'll expect to hear a murmur in the pulmonic region as well with ASD. So this is a picture that we looked at earlier and this is a picture that we are reiterating what we are going to do throughout this lecture series is then delineate and distinguish each valvular heart disease and you will be in good hands. 04:02 Trust me.
About the Lecture
The lecture Aortic Stenosis: Auscultation Areas by Carlo Raj, MD is from the course Valvular Heart Disease: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following areas can reveal the murmur of aortic stenosis?
- 2nd intercostal space at the right upper sternal border
- 2nd intercostal space at the left upper sternal border.
- 5th intercostal space at the right lower sternal border.
- 4th intercostal space at the left lower sternal border.
- 5th intercostal space in the left midclavicular line
Author of lecture Aortic Stenosis: Auscultation Areas

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I love the domain of the subject that the doctor has, the explanation of the subject was good
