Playlist
Show Playlist
Hide Playlist
Conjugated Hyperbilirubinemia


-
Slides Conjugated Hyperbilirubinemia and Liver Diseases Pediatrics.pdf
-
Download Lecture Overview
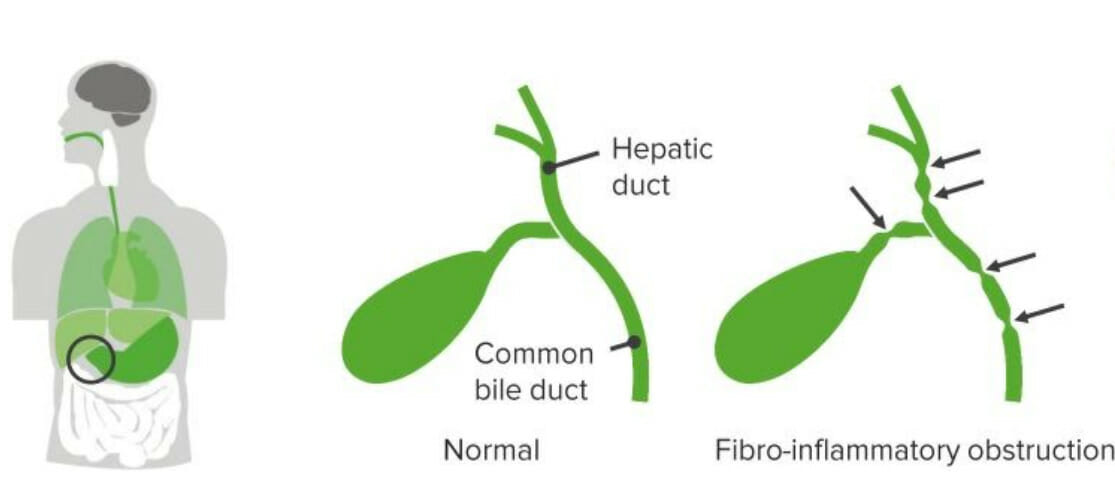
00:02 In this lecture, we’re going to discuss conjugated hyperbilirubinemia and liver diseases in children. 00:09 This happens every now and then, a child is born who’s a little bit yellow and it turns out they’re having conjugated rather than unconjugated hyperbilirubinemia. 00:19 And it’s important in these conditions to know what exactly is going on. 00:25 So the definition of conjugated hyperbilirubinemia is more than 1 mg per deciliter, if the total bilirubin is less than 5. 00:37 Or more than 20% of your total bilirubin if the total bilirubin is more than 5. 00:44 So we have to remember that 5 cut off in terms of how we define hyperbilirubinemia. 00:52 The differential diagnosis for a child with conjugated hyperbilirubinemia is generally either an extrahepatic problem where the bile can’t get out or an intrahepatic problem. 01:06 Elevated conjugated bilirubin is never normal in a neonate and that’s an incredibly important fact. 01:13 Unconjugated or indirect hyperbili is very common and we see it all the time. 01:19 But when it’s conjugated, there is definitely a problem. 01:23 So when you see a patient with conjugated hyperbilirubinemia, it’s important to take a good history. 01:30 Family history is critical because there are inherited syndromes where children are more prone to liver disease. 01:38 Asking about consanguinity is always important as well because obviously with consanguineous families, recessive disorders are more likely to show up. 01:48 Understanding if there were any pregnancy complications can be helpful as well as some of these conditions are syndromic and there may be a problem. 01:56 Or even more likely, the mother may have obtained an infection during pregnancy. 02:02 Some of the TORCH infections can cause hepatitis in children. 02:08 Asking about the delivery and whether there were any complications and certainly whether there were any infectious exposure to the child are important. 02:16 It’s critical to do a good physical exam on these children. 02:19 Specifically, knowing their growth parameters and plotting them on a growth curve, both height, weight and head circumference is critical to understanding how this child is developing and if their hepatic disease is affecting them or if this is part of a syndromic situation. 02:36 Understanding vital signs and making sure they’re normal are critical. 02:39 And of course, a skin evaluation will give you a sense of just how bad the hyperbilirubinemia might be prior to actually getting the lab value. 02:49 Conjunctival icterus is common in these patients and it may be how you find it. 02:54 The best place to look for jaundice may be under the tongue, around the frenulum area. 03:01 Patients, if they have a cardiac condition and there are some conditions like Alagilles which we’ll talk about in a bit, that are associated with cardiac findings. 03:12 So understanding a cardiac murmur and listening for one is important as well. 03:17 The abdominal exam is of course critical. 03:20 Especially feeling for that liver edge or doing the scratch test, which may be an even better way to assess for hepatomegaly in children. 03:30 Of course, labs are the mainstay and so obtaining a bilirubin is important. 03:36 Remember especially in babies, you can’t just get a total bilirubin, you need to break it down into direct and indirect bilirubin. 03:45 That’s because although most children with neonatal jaundice have elevated indirect or unconjugated bilirubin. 03:52 The children with direct or conjugated hyperbilirubinemia can't be missed because they should not be given phototherapy. 04:00 Otherwise, they may develop bronze baby syndrome. 04:04 Of course, checking the liver function test is important and don’t forget the GGT, which is useful for assessing the biliary tree because many if these children have abnormalities of the biliary tree. 04:18 Synthetic function tests like PT, PTT and INR are important for understanding whether the liver is working. 04:26 It’s not enough to just know it’s inflamed, we also want to know whether it’s functioning correctly.
About the Lecture
The lecture Conjugated Hyperbilirubinemia by Brian Alverson, MD is from the course Pediatric Gastroenterology.
Included Quiz Questions
If you light a baby with lights and they have conjugated hyperbilirubinemia, what might happen?
- Bronze baby syndrome
- Dehydration
- Improvement of bilirubin levels
- Increased melanin production
- Hyperthermia
A newborn with jaundice is found to have increased GGT levels. What is this indicative of?
- Abnormality of biliary tree
- Hemolysis
- Hepatitis
- Erythroblastosis fetalis
- Physiologic rise
Author of lecture Conjugated Hyperbilirubinemia

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Important topic in pediatrics. Very clear explanations. Helps to understand the topic very much. Thank you!
