Playlist
Show Playlist
Hide Playlist
Case: 68-year-old Man with Progressive Altered Mental Status

-
Slides Head Trauma.pdf
-
Download Lecture Overview
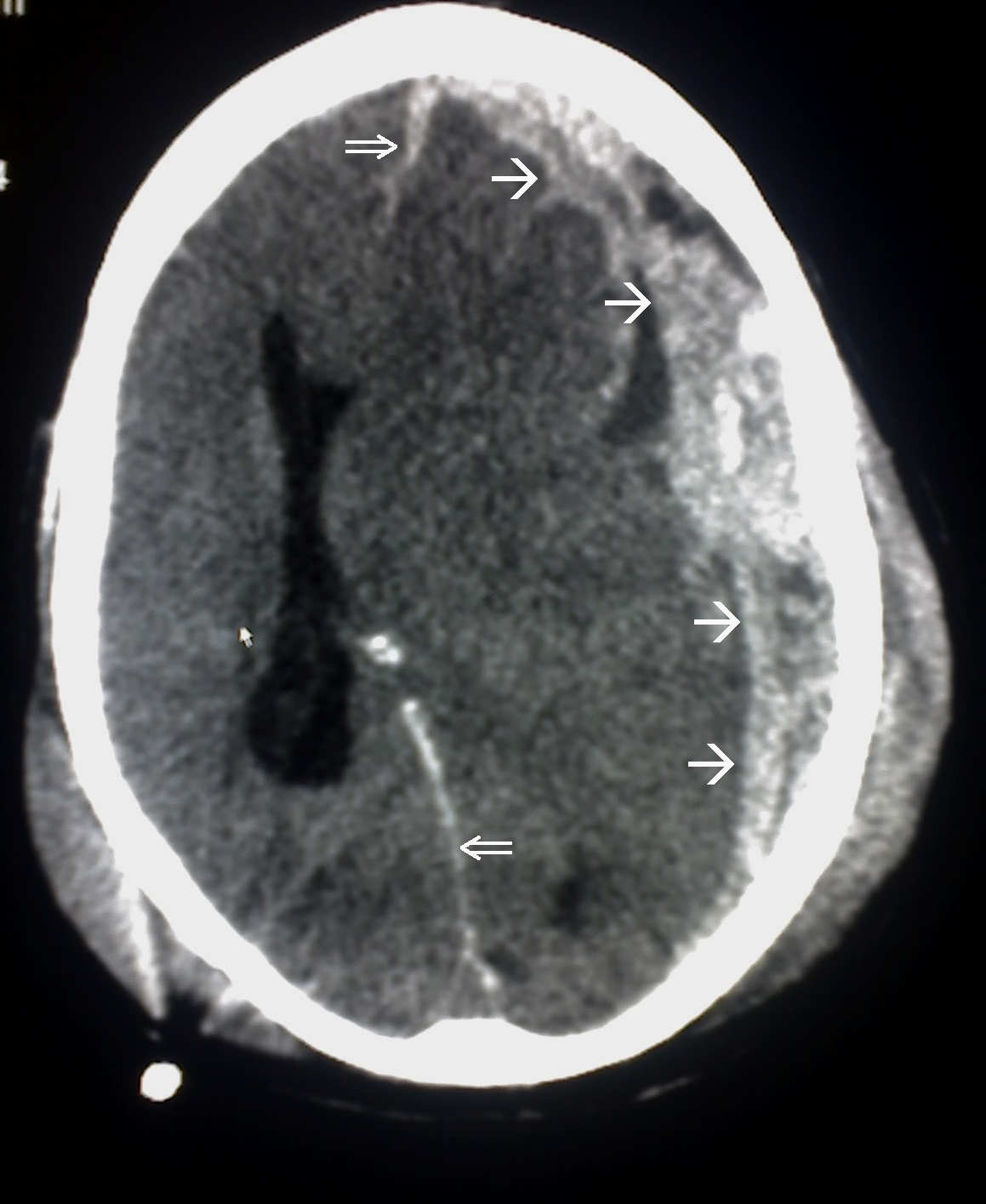
00:01 In this talk, we're going to review head trauma and begin with an orientation for what is head trauma and how do we think about it. 00:11 Let's start with a case. 00:13 This is a 68 year-old man with no significant past medical history who presents to the emergency department with progressive altered mental status. 00:22 The patient initially fell from a small ladder in his home 4 days ago. 00:27 His family says that he appeared normal immediately after the fall. 00:30 And over the past few days, he has become progressively weaker, began to trip with his right leg and uses his right arm less. 00:38 Today, the patient became progressively more confused and has not been speaking. 00:44 On examination, he is awake and his eyes are open spontaneously. 00:48 He has a left gaze preference, he prefers to look left. 00:51 But is able to look past the midline to the right. 00:55 He moves his left hemibody with full strength but has significant or severe right hemiparesis. 01:00 He's weak on the right side of the body, and is only able to withdraw to pain. 01:06 So how do we think about this case? And let's talk about some of the key features. 01:10 First, there was an initial trauma. 01:11 He fell and could a sustained some type of head injury. 01:15 Second, the course has been progressive over time. 01:19 It began with this injury and it's progressively become more confused, develop this right hemiparesis and now with significant worsening prior to his presentation. 01:29 And then the last is this, the patient has a right hemiparesis and the localization of this problem is to the left side of the brain. 01:38 So what's the most likely diagnosis? Has this patient suffered an epidural hematoma, subdural hematoma, a subarachnoid hemorrhage, or is this the presentation of glioblastoma? Well, this doesn't sound like glioblastoma. 01:54 The patient has a subacute course after a fall. 01:58 Patients with malignant brain tumors can present over the course of several weeks. 02:02 But this presentation is much more suggestive of a traumatic brain injury than a neoplasm. 02:11 This is not the typical presentation of an epidural hematoma. 02:15 With epidural hematomas, we often hear of a lucid interval, an initial trauma where the patient has slightly altered immediately afterwards, followed by a period of normalization. 02:26 And then typically within hours or less than a day, the patient presents with progressive neurologic decline. 02:31 And this has been a more gradually progressive course over several days, which is not typical for what we hear with an epidural hematoma. 02:40 This also is not the typical presentation of subarachnoid hemorrhage. 02:44 The patient has a subacute progressive course. 02:48 And with subarachnoid we often worry about or hear about a thunderclap headache or a severe rapid onset headache with evidence of meningeal irritation, nausea, vomiting and increased intracranial pressure which we don't have in this case. 03:03 And so this is really the typical presentation of a patient who has a subdural hemorrhage. 03:08 An initial traumatic event, followed by gradual progression of neurologic symptoms and focal neurologic deficits on exam that result from the area where the hemorrhage has irritated the cortex.
About the Lecture
The lecture Case: 68-year-old Man with Progressive Altered Mental Status by Roy Strowd, MD is from the course Head Trauma.
Included Quiz Questions
In an elderly patient who recently suffered head trauma, what is the most likely cause of progressive focal neurologic deficits?
- Subdural hematoma
- Epidural hematoma
- Subarachnoid hemorrhage
- Glioblastoma
- Acute ischemic stroke
In a patient who recently suffered a head injury and developed a "lucid interval" before rapid cognitive decline, which diagnosis would be most likely?
- Epidural hematoma
- Subdural hematoma
- Subarachnoid hemorrhage
- Glioblastoma
- Acute ischemic stroke
In a patient who suddenly developed "the worst headache of [their] life" in the absence of trauma, followed by rapid cognitive decline, which diagnosis would be most likely?
- Subarachnoid hemorrhage
- Subdural hematoma
- Epidural hematoma
- Glioblastoma
- Acute ischemic stroke
Author of lecture Case: 68-year-old Man with Progressive Altered Mental Status

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
