Playlist
Show Playlist
Hide Playlist
Massive Hemothorax

-
Emergency Medicine Pulmonary Trauma.pdf
-
Download Lecture Overview
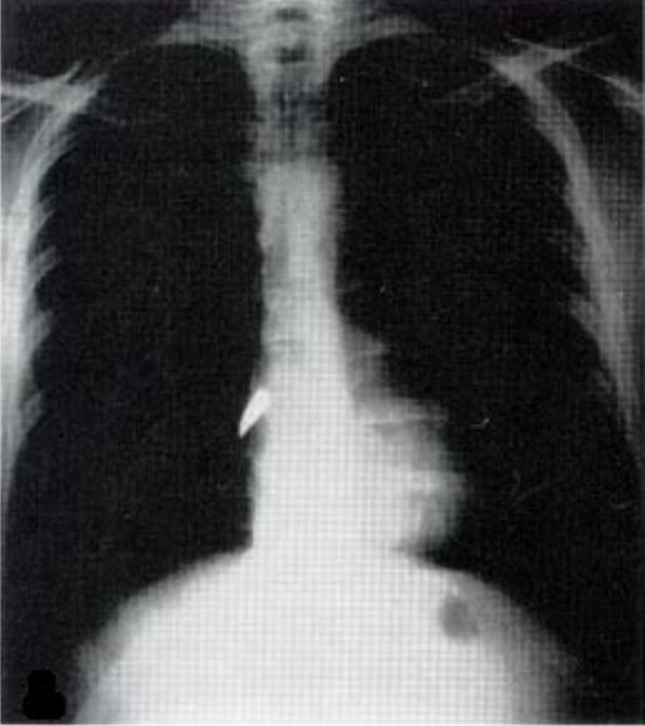
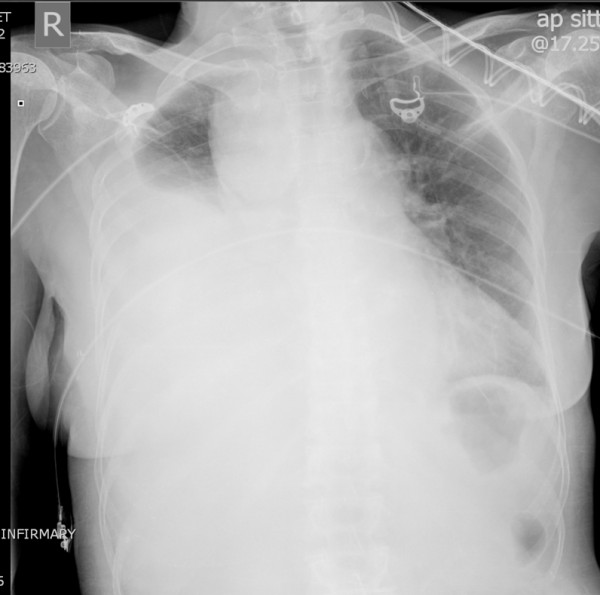
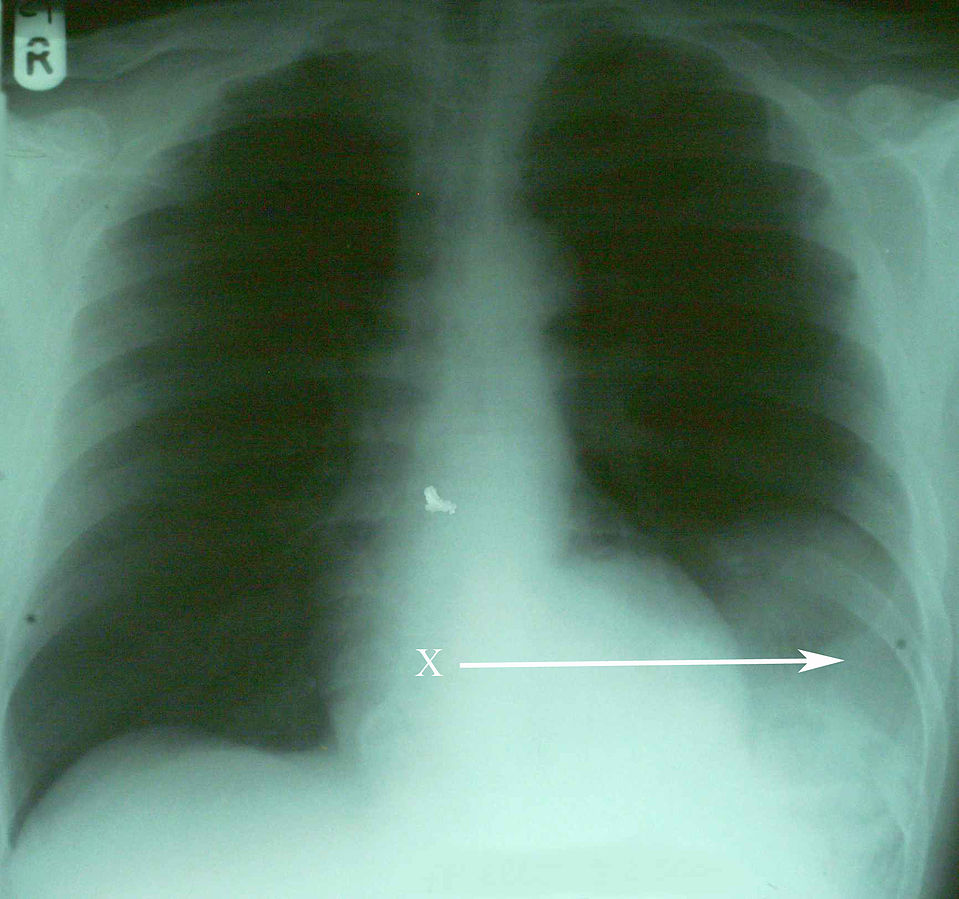
00:01 Alright, the last diagnosis to talk about is massive hemothorax. 00:05 So hemothoraces are defined as any collection of blood in the pleural space. 00:13 So if you’ve got blood in the pleural space which normally shouldn’t have anything in it, you’ve got a hemothorax. 00:18 There’s a number of different injuries that can lead to hemothorax so injury to the lung parenchyma itself is the most common. 00:27 Fortunately, the lungs are highly vascularized but you’re generally talking about pretty small vessels with parenchymal injuries so these will typically clot off and heal themselves and the bleeding into the pleural space will be self limited. 00:42 By contrast, if you have injury to the intercostal arteries, the mammary arteries or the great vessels, these are larger vessels that may or may not be able to clot themselves off and you’re typically gonna have more sustained bleeding that can potentially be life threatening. 00:59 Now, hemothorax does impair ventilation especially if it’s a large quantity hemothorax so if you’ve got one hemothorax completely filled with blood, that is gonna impair ventilation but only on the affected side. 01:11 It is possible to get a tension hemothorax. 01:16 This really only occurs with large vessel injuries, specifically arterial injuries, because arterial bleeding is pushed into the pleural space under pressure so it can actually increase the pressure in the thoracic region and cause tension physiology. 01:37 This is very rare. 01:39 I’ve actually never seen a case of this myself in practice but it is theoretically possible and something for you to be aware of. 01:45 So on physical exam, you probably will see some signs of hemorrhagic shock for your patient. 01:52 Each hemothorax holds a liter to a liter and a half of blood depending on the size of the person so you can imagine that you’re gonna get some signs and symptoms associated with bleeding if you have that much blood in your chest wall. 02:05 You’re gonna typically have absent or decreased breath sounds on the affected side and if you do percuss the lungs you’re gonna find that they’re dull because instead of being filled with air they’re now filled with fluid. 02:17 Your chest x-ray’s your best initial test for this. 02:21 Upright chest x-rays are better when you can do it safely because it will allow you to see the layering of the blood and will show you how much blood roughly is in the chest cavity. 02:32 But if you can’t sit your patient up safely, a supine test will also tell you there’s a hemothorax. 02:38 It won’t let you estimate the quantity as well because the blood will layer out if the patient is supine so you usually just see diffused haziness or opacity on the affected side. 02:50 A CT scan of the chest offers you a little bit more of a definitive diagnosis and allows you to more reliably quantitate how much blood is in the pleural space. 03:02 You can see the arrow on this image marks the large hemothorax that’s present on the patient’s left hand side. 03:09 So what do we do for hemothoraces? Generally, these patients are all gonna need chest tubes and the reason for that is one, we wanna monitor ongoing bleeding, right? We can’t be sending our patients back to the CT scanner every half hour so we need a way of knowing if their hemothorax is improving, expanding, or staying the same. 03:29 So we wanna monitor their bleeding by looking at their chest tube output and we also wanna allow that injured lung to re-expand and heal. 03:37 Patients with hemothoraces do sometimes need to go to the operating room for thoracotomies and that occurs when they have large volumes of blood in the pleural space and might have vascular injuries that need repair in order to stop bleeding. 03:54 So anytime you get 1500 cc of blood out on initial chest tube insertion, you wanna go to the operating room, that’s a sign again that you have a vascular injury rather than just injury of the pulmonary parenchyma. 04:06 And anytime you have persistent brisk bleeding overtime, so more than 200 cc of blood per hour for 3 or more hours, again, that’s a sign that you’ve got a vascular injury that’s not able to clot itself off and you need to consider operative management. 04:24 So patients with massive hemothorax may be hemodynamically unstable, they may have whiteout on their chest x-ray. 04:32 These massive hemothorax patients so they have complete filling of one hemothorax with blood are much more likely to have vascular injuries and they’re much more likely to need surgery but we’re always going to place a chest tube in these patients and define whether or not their hemothorax require surgery based on their chest tube output as we just discussed. 04:56 So just remember, ABCs first, right? If you’ve got a massive hemothorax, that’s a sign that you’ve got internal bleeding somewhere in the chest and you potentially need to resuscitate your patient so don’t just focus on the lungs, focus as well on the need for adequate IV access, volume resuscitation, et cetera. 05:16 Severe respiratory distress is actually uncommon in these patients because the other lung will usually meet the patient’s physiologic needs from a respiratory standpoint, however, the blood loss might be significant and patients often need volume resuscitation. 05:32 In rare cases, especially for patients with underlying lung disease, you may end up needing to give them some respiratory support even intubate and mechanically ventilate them, but most often the complications associated with massive hemithoraces
About the Lecture
The lecture Massive Hemothorax by Julianna Jung, MD, FACEP is from the course Trauma (Emergency Medicine).
Included Quiz Questions
What is the most common bleeding source in hemothorax?
- Lung parenchymal injury
- Intercostal artery injury
- Internal mammary artery injury
- Great vessel injury
- Hilar injury
What is the best initial test in the diagnosis of hemothorax?
- Chest x-ray
- Chest ultrasound
- CT scan
- MRI
- CT angiography
Thoracotomy is indicated when the volume of blood initially drained during chest tube insertion is at least how much?
- 1500 cc
- 200 cc
- 500 cc
- 800 cc
- 1000 cc
What is the definitive test in diagnosing hemothorax?
- Chest CT scan
- Chest x-ray
- Chest ultrasound
- MRI
- CT angiography
Author of lecture Massive Hemothorax

Julianna Jung, MD, FACEP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
