Playlist
Show Playlist
Hide Playlist
Cardiac Case: 68-year-old Woman with Murmur and Abnormal Heart Valve

-
Cardiac Case 68-year-old Woman with Murmur and Abmornal Heart Valve.pdf
-
Download Lecture Overview
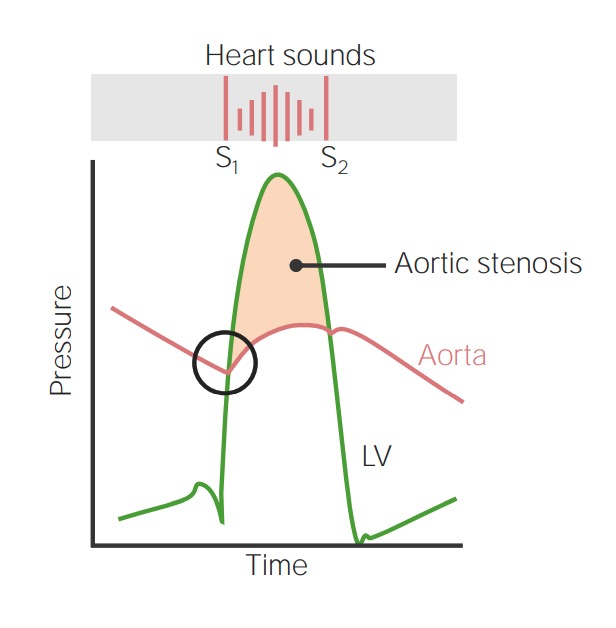
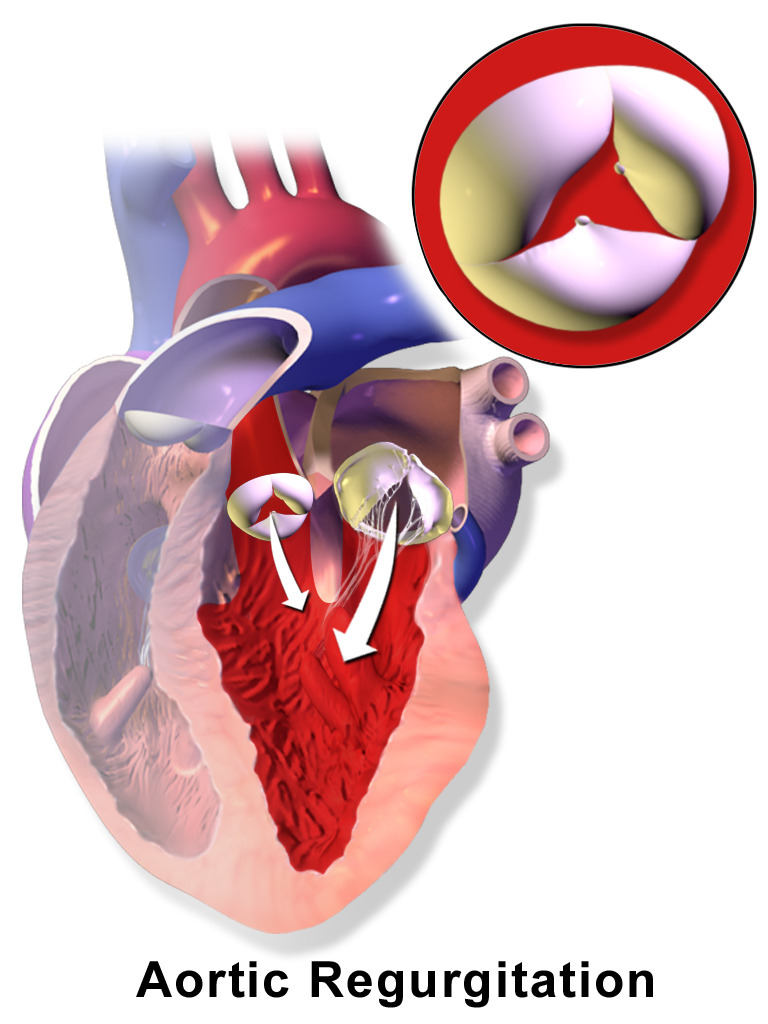
00:01 A 68-year-old woman is referred to you for evaluation of a murmur. 00:05 She tells you she was diagnosed with a murmur and an abnormal heart valve as a young woman. 00:10 She takes antibiotics before visiting the dentist but says she feels well she walks two miles every day without symptoms. 00:17 Her physical exam show something interesting. 00:21 First of all, her systolic pressure is a little bit elevate at 145 and her diastolic pressure is very low at 48 so there are several things that could go this - very stiff arteries can give you this wide pulse pressure as could a valvular lesion aortic insufficiency or also called aortic regurgitation. 00:39 The pulse is regular at a reasonable rate, fingertip oxygen saturation normal. 00:44 JVP is normal, jugular venous pulse that is quite normal, carotid pulse is very brisk. 00:50 The brisk carotid pulse and the wide pulse pressure are suggesting to be this patient may have aortic insufficiency. 00:57 Her lungs are clear so there’s not heart failure and heart sounds, she has a grade 2 systolic ejection murmur and a grade 2 diastolic murmur heard at the upper right sternal border and no S3 again consistent with an aortic regurgitation. 01:14 The systolic murmur doesn’t mean she has an aortic stenosis it’s just because of the increased flow that goes across an abnormal aortic valve during systole so let’s imitate that. 01:25 So normal heart, lub-dub, lub-dub, lub-dub. Here’s her: lub-shshdub-whoo, lub-shshdub-whoo, lub-shshdub-whoo. 01:37 So you heard there's two murmurs the systolic ejection murmur because of turbulence from the large flow going across the aortic valve and then the diastolic blowing murmur of aortic insufficiency. 01:49 She has no peripheral edema so there’s nothing in the exam or the history that suggest heart failure. 01:53 So what's the critical factors here? She has a history of heart disease so you’re gonna be looking for a valvular heart disease and of course her physical exam shows you a wide pulse pressure as well as signs of aortic valve disease. We do a chest x-ray and then we’ll do a Doppler echo. 02:13 Here’s the chest x-ray - her left ventricle is enlarged, you can see again the apex is pushing out towards the chest wall but the lungs are clear and in the aortic regurgitation also one has an enlarged aortic route and you can see that on this view of the chest x-ray, the dilated ascending aorta. 02:34 And here’s the Doppler, you can see in the rainbow color area a large amount of aortic regurgitation flowing across the aortic valve. 02:44 Large regurgitant jet flowing across an abnormal aortic valve. 02:50 Other options, her blood test are all normal, kidney functions normal which is good, so the conclusion of the echo is that she has moderately severe aortic insufficiency, she has a bicuspid aortic valve. 03:02 One percent of the population is born with a two cusp aortic valve rather than a three cusp and the bicuspid aortic valve wears out early, sometimes associate also with the ascending aortic aneurysm or dilation of the ascending aorta. 03:17 The left ventricle is enlarged but has normal ejection fraction so normal functioning and she has an enlarged aortic route which is quite common with a bicuspid aortic valve. 03:28 The bicuspid valve can go on to either stenosis or regurgitation with time, in this case it went on to aortic regurgitation and the left ventricle dilates in order to pump the larger end diastolic volume into the aorta because of the blood that flows back into the left ventricle during diastole with the aortic regurge. 03:49 For symptomatic patients with severe aortic regurgitation. 03:52 Surgery is recommended after a period of intense medical therapy for heart failure when the patients have reduced ejection fraction or health risk. 04:01 And this includes, of course, diuretics as well as vasodilators with either an ACE inhibitor, angiotensin receptor blocker or with an ARNI. 04:12 As we talked about that combination of ARB, as well as a blocker for the breakdown of atrial naturally peptide. 04:23 It's the same as patients with other patients with HefRef. these or die leaders are particularly important in aortic regurgitation because they encourage forward flow as opposed to retrograde flow. 04:37 This patient's lungs are clear, so there's not any symptoms of heart failure and the heart sounds are normal. 04:43 She has a grade two systolic ejection murmur and a grade two diastolic murmur. 04:47 Her to the left sternal border at the third or fourth intercostal space and no S3. 04:52 Again, consistent with aortic regurgitation, but ventricular function is not terrible at this point. 04:59 If the aortic regurgent volume is very large left ventricular failure can eventually develop and that requires replacement of the aortic valve. 05:09 Using prophylactic antibiotics for dental work or surgery has been a controversial area. 05:17 Some countries have actually shown when they stop doing this prophylaxis, the incidence of endocarditis went up. 05:25 This was not the case in the United States, but there are still many practitioners who prophylaxis patients with bicuspid aortic valves with antibiotics. 05:35 There will probably never be a double blind, randomized controlled trial here. 05:39 So again, this is often shared decision making with the patients. 05:45 I tend to use prophylactic antibiotics with patients with bicuspid aortic valves, but many of my colleagues do not.
About the Lecture
The lecture Cardiac Case: 68-year-old Woman with Murmur and Abnormal Heart Valve by Joseph Alpert, MD is from the course Cardiovascular Cases.
Included Quiz Questions
A 68-year-old woman presents for evaluation of a murmur. She states that a murmur and "an abnormal heart valve" were diagnosed when she was a young woman. She takes antibiotics before visiting the dentist. She reports feeling well and walks 2 miles every day without symptoms. A grade 2/6 systolic ejection murmur and grade 2/6 high-pitched diastolic murmur are heard best at the upper right sternal border during cardiac auscultation. After the appropriate physical examination and diagnostic tests, heart failure is excluded. Which of the following will most likely be detected during the physical examination of this patient?
- Isolated systolic blood pressure
- Jugular venous distention
- Crackles
- Low fingertip oxygen saturation
- Pulsus parvus et tardus
A 68-year-old woman presents for evaluation of a murmur. She states that a murmur and "an abnormal heart valve" were diagnosed when she was a young woman. She takes antibiotics before visiting the dentist. She reports feeling well and walks 2 miles every day without symptoms. A grade 2/6 systolic ejection murmur and grade 2/6 high-pitched diastolic murmur are heard best at the upper right sternal border during cardiac auscultation. Otherwise, her physical examination results are normal. Which of the following will most likely be found during workup?
- Left ventricular dilation
- Regurgitant jet across the mitral valve
- Calcified aortic valve
- Ascending aortic aneurysm
- Low left ventricular ejection fraction
Which of the following heart murmurs is most suggestive of aortic valve insufficiency?
- A diastolic murmur that is best heard at the Left 3rd intercostal space
- A holosystolic murmur that is best heard at the left lower sternal edge.
- A crescendo-decrescendo systolic murmur that is best heard over the left second intercostal space.
- A crescendo-decrescendo systolic murmur that is best heard over the right second intercostal space.
- An early diastolic murmur that is best heard at the heart apex.
Author of lecture Cardiac Case: 68-year-old Woman with Murmur and Abnormal Heart Valve

Joseph Alpert, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
