Playlist
Show Playlist
Hide Playlist
Dopamine Agonists and Prolactinomas in Pregnancy

-
Slides ProlactinandPituitaryDisorders ReproductiveEndocrinology.pdf
-
Download Lecture Overview
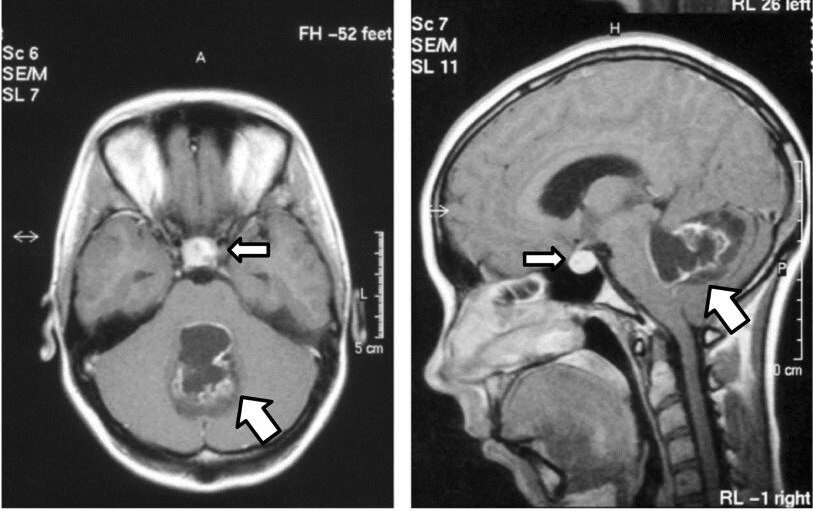
00:00 Now I’d like to call your attention to the dopamine agonist that we traditionally use. Bromocriptine has been around for quite some time. It is successful in normalizing prolactin levels or causing return of ovulatory menses in 80 to 90% of females. Cabergoline has a higher efficacy in normalizing prolactin and a higher frequency of tumor shrinkage and it’s the preferred agent of the American Endocrine Society. It has a longer half-life and has bi-weekly dosing. However, a clinical caveat is that we tend to use bromocriptine because it’s been used in pregnancy for quite some time. 00:38 However, it’s not as well tolerated as cabergoline. One clinical pearl is that you can have the patient take this medication before bedtime. However, I’d like to tell you that dopamine agonist don’t always work. However, we should always try to maximize the dosages of dopamine agonist before we refer for any type of surgery. Transsphenoidal surgery and radiation are alternatives. 01:06 I would now like to discuss prolactinomas in pregnancy. You can have a microprolactinoma or a macroprolactinoma before you become pregnant. That should not be a contraindication to pregnancy and actually once the patient is on dopamine agonist, she may resume ovulation and become spontaneously pregnant. If she doesn’t desire to do so, remember to give her some type of contraceptive. However, once the woman becomes pregnant, she should stop her dopamine agonist. 01:36 Bromocriptine does not cross the placenta and we think it’s safe in pregnancy. However, there is very little safety data on cabergoline. If patients become symptomatic, then we should reinstitute dopamine agonist. This is preferable to surgery especially during these 9 months of gestation. We should not be checking prolactin levels in pregnancy, we should just follow the woman for her symptoms. Remember that prolactin is already elevated during pregnancy. Let’s now talk about what happens to micro- and macroadenomas during pregnancy. If a patient has a microadenoma less than 10 mm and she doesn’t have any prior therapy with a dopamine agonist, then about 2.7% of those patients may have symptomatic enlargement according to one study. 02:28 In terms of macroadenomas larger than 10 mm, if that patient has no prior therapy then about 22.9% of those patients will have some symptomatic enlargement. Macroadenomas that had been treated with a dopamine agonist prior to pregnancy will actually have a reduced number of patients who have symptomatic enlargement at 4.8%. So remember, dopamine agonist are indicated before pregnancy. Let’s now review prolactinomas and breastfeeding. There is no evidence that breastfeeding stimulates tumor growth. For women who wish to breastfeed, we should withhold dopamine agonist until they have weaned the child. The American Academy of Pediatrics actually recommends that a child be breastfed for 12 months. Let’s now review a case. A 28-year-old G0 presents to your clinic with a history of missing her periods. She doesn’t think she is pregnant but she is not sure. When you take a history, her history reveals no medications except a multivitamin. Remember antipsychotics and neuroleptics can be culprits in hyperprolactinemia. When you do a physical exam, it’s unremarkable. Is that a problem? Actually, no. Many patients don’t display galactorrhea. 03:46 When you do a urine pregnancy test and a serum beta-hCG, they’re both negative. So you successfully ruled out pregnancy in this patient. What else do you want to know? Well, you should check a TSH. 04:05 This patient’s TSH is normal. Her prolactin though is elevated. It varies from institution to institution but usually it’s between 20 to 25 as a high normal. Anything above that would be elevated. You ask the patient was she fasting? Was this taken in the a.m.? Does she have any undue stress? She says,”Yes, she was fasting. Yes, it was taken in the a.m. and no undue stress." Should you believe this prolactin? If you recall from early in the lecture, the answer is yes. What’s your next step? Your next step would be to image, image her hypothalamic, pituitary region. Here, you see there is a mass. This is an MRI with a T1 weighted image. What’s your differential diagnosis? Well if you thought microprolactinemia or micro, that’s a good differential diagnosis. Now let’s talk about a 31-year-old woman who has never had her period. That’s problematic. This should’ve been discovered long ago, hopefully, by a pediatrician or a family doctor. This patient actually was in a motor vehicle accident as a teenager. She had head trauma as a result. Hmm. This makes sense now. If you need to review the axis of the hypothalamic pituitary, just skip backwards and you’ll see it. This patient has been on oral contraceptive pills since the diagnosis of panhypopit. She wants to now get pregnant. How would you treat her? I’ll give you a second. 05:58 Well, remember, her pituitary is non-functioning. Therefore, her gonadotrophs are not firing. 06:05 They’re not making FSH and LH. So what would you give her now? If you guessed FSH and LH with an hCG trigger for ovulation, you guessed right. I just want to briefly review something called the hook effect. What if you suspected elevated prolactin in a patient and it was negative when you sent her for a serum blood test? Sometimes it can be a large molecule called macroprolactinemia but sometimes the prolactin can be so elevated that the test actually is negative. How can that that be? It’s something called the hook effect. This happens with high serum beta-hCG as well. 06:47 What happens is that you’re analyzing a hormone that is in such high level that it actually binds all of the antibody that would actually show a signal. That antibody is bound and it can’t bind to the immobilize antibody here in the well. When this happens, it may show up as a false negative. 07:09 If there is more analyte, then the hormone that you are testing, then usually you can get a sample. So typically you want the lab to do a dilution and that will eliminate this effect. 07:22 Thank you for listening and good luck on your exam.
About the Lecture
The lecture Dopamine Agonists and Prolactinomas in Pregnancy by Lynae Brayboy, MD is from the course Reproductive Endocrinology. It contains the following chapters:
- Dopamine Agonists & Prolactinomas in Pregnancy
- Case Studies
Included Quiz Questions
Which of the following syndromes can be associated with a pregnant patient with prolactinoma?
- MEN -1
- MEN - 2A
- MEN -2B
- Cowden syndrome
- Turcot syndrome
Which of the following is NOT a treatment used for macroprolactinomas?
- Dopamine antagonists
- Bromocriptine
- Cabergoline
- Transsphenoidal surgery
- Radiation
A 32-year-old lady with primary infertility is diagnosed with a micro prolactinoma. She was started on bromocriptine and she got pregnant. Bromocriptine was discontinued. About 12 weeks into the pregnancy she complains of headaches. Her blood pressures are normal. What is the next best step of management?
- Restart bromocriptine
- Perform transsphenoidal surgery
- Provide radiation
- Check prolactin levels to confirm increase in size
- Prescribe cabergoline
Which of the following is FALSE regarding management of prolactinomas?
- Minimize the dose of dopamine agonists before referral to surgery.
- MRI can be performed to visualize prolactinomas in pregnant women.
- Prolactin level in pregnancy with prolactinoma is not useful for the diagnosis.
- Breastfeeding is contraindicated in patients who are on dopamine agonists.
- Radiation is NOT a therapeutic option for macroadenomas in patients who are pregnant.
Which of the following is FALSE regarding hook effect?
- Repeated measurements of the hormone levels will provide accurate measurement.
- Dilution helps to obtain the appropriate values in hormones that are affected by a hook effect.
- Hook effect is not restricted only to prolactin hormone.
- The hormone is in high concentrations that it gets attached to the antibodies that provide a signal and is unable to bind to the immobilized antibodies on the surface.
- Hook effect is when the hormone is so largely elevated that the test results as false negative.
Author of lecture Dopamine Agonists and Prolactinomas in Pregnancy

Lynae Brayboy, MD
Customer reviews
2,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
1 |
| 1 Star |
|
0 |
The lecture is not clearly structured, and not easy to follow, often have to pause to figure out what is being said. Look at Dr. Raj's lectures for better teaching strategies
