Playlist
Show Playlist
Hide Playlist
Pericarditis: Signs and Symptoms


-
Slides Pericarditis InfectiousDiseases.pdf
-
Download Lecture Overview
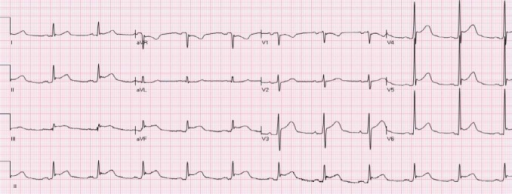
00:01 How do the patients present? Well, most of them have rather striking aching precordial chest pain. 00:10 Of course, that makes us worry about heart disease. But this is quite different from heart disease type pain. 00:19 The pain itself may be slightly similar in the sense that it’s aching. But this kind of pain is actually aggravated by the patient lying back. The patient by gravity, the pericardium is stretched a little bit by lying supine. That’s why the pain may get worse. Certainly, when they cough, they jar the pericardial sac and that may make the pain worse. Of course, deep inspiration produces pain because as the lungs expand, they put pressure on the inflamed pericardium. You might be able to predict what would relieve it. 01:00 Having the patient sit upright especially leaning forward would perhaps relieve it to some degree. 01:08 It doesn’t go away but it does ease somewhat. When they splint their respirations, in other words, when they try not to take a deep breath, that may give them some relief. 01:23 The other thing is the radiation of pericardial pain actually is into the neck region. 01:28 That can be the case with a myocardial infarction pain but the difference is that a pain of myocardial infarction stays unchanged with changing position. 01:36 So, maneuvers may relieve the pericardial pain but not generally so with acute MI. 01:42 Furthermore, the patients with acute MI are usually dyspneic. They’re usually sweating. 01:47 They may have labile blood pressure. They will have a characteristic cardiac examination. 01:56 On exam, and I think physicians today are not doing what I would call the world class exam anymore, but if you listen carefully in most patients with pericarditis, you can hear what we call a pericardial friction rub. That’s either a scratchy or leathery sound that’s got three components. 02:20 The first component is during atrial contraction. That would be just before systole. 02:27 The next component would be that scratching sound during ventricular systole. Then early in diastole during rapid ventricular filling, you get another scratching sound. So, it’s kind of a three component rub that's not affected that much by inspiration. The other thing is that the heart sounds in pericarditis, if there’s a sizable accumulation of fluid in the pericardium, the heart sounds can be rather distant or muffled. 03:00 On X-ray, what we find is an enlarged cardiac silhouette. But it’s not an enlarged heart. 03:12 It’s just representative that there’s fluid present in the pericardium giving the cardiac silhouette sort of a water bottle sized heart. It’s rather huge. 03:26 A massive Pericardial effusions or rapid accumilation of fluid can lead to pericardial tamponade, which is a fatal complication. 03:34 Tamponade is characterized by the Beck's triad, which includes Hypotension, distended neck veins and distant, muffled heart sounds. 03:42 And may produce pulsus paradoxus. 03:46 This is kind of a misnomer. Normally, the blood pressure drops slightly during inspiration. 03:55 But it usually doesn’t drop by more than 10 mmHg. In pericardial tamponade with pulsus paradoxus on inspiration, the pressure drops substantially more than 10 mmHg. 04:18 The electrocardiogram is pretty characteristic in acute pericarditis. 04:21 The main thing to notice in these leads is that there is elevation of the ST segment in essentially all leads and occasionally depression in AVR, and also depression in the PR segment. 04:31 So, notice the elevation of the leads of the ST segment in these leads. 04:35 This is different from the EKG changes in pericardial effusion, where you find electrical alternans and low amplitude EKG. 04:43 Some laboratory findings may show you an increased CPK and troponin I, even though it’s not the heart that’s severely damaged by this process. The electrocardiogram is pretty characteristic in acute pericarditis. The main thing to notice in these leads is that there is elevation of the ST segment in essentially all leads and occasionally depression in AVR. So, notice the elevation of the leads of the ST segment in these leads.
About the Lecture
The lecture Pericarditis: Signs and Symptoms by John Fisher, MD is from the course Cardiovascular Infections.
Included Quiz Questions
What helps relieve pain caused by pericarditis?
- Leaning forward while sitting upright
- Deep breathing
- Laying down
- Rest
- Arching the back
Which cardiac exam finding is commonly observed in a patient suffering from pericarditis?
- Friction rub
- Amplified heart sounds
- Mid-systolic click
- Murmur lower in amplitude on inspiration
- Holosystolic murmur
What is seen on chest x-ray imaging of acute pericarditis?
- Enlarged cardiac sillhouette
- Lateral shift in the cardiac sillhouette
- Narrowing of the cardiac silhouette
- There are no radiological findings in pericarditis
- Aortic arch enlargement
What is a typical electrocardiogram finding in acute pericarditis?
- ST segment elevation in most leads
- ST segment elevation in lateral leads
- T wave depression in anterolateral leads
- PR interval reduction
- ST segment depression in all leads
Author of lecture Pericarditis: Signs and Symptoms

John Fisher, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
