Playlist
Show Playlist
Hide Playlist
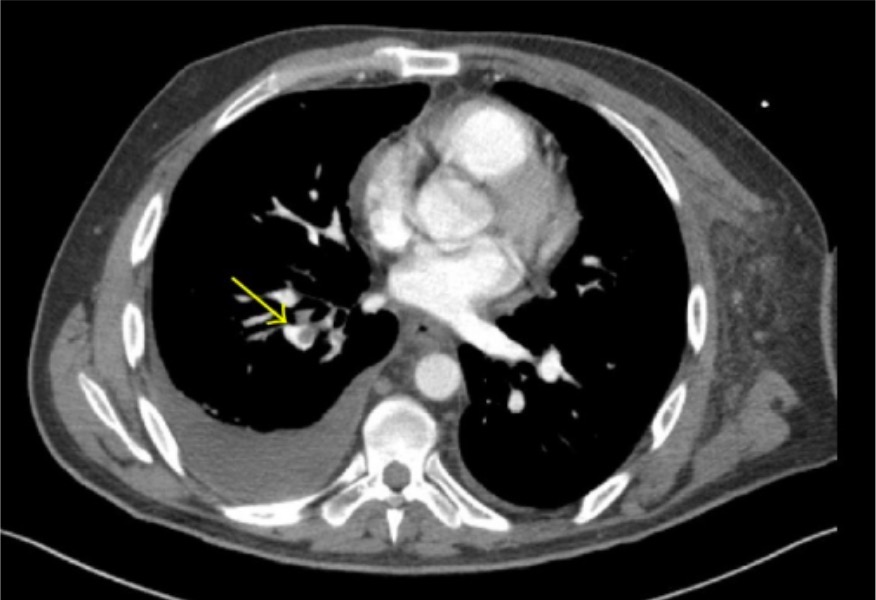
Pulmonary Emboli

-
Slides 08 VascularDiseases RespiratoryAdvanced.pdf
-
Download Lecture Overview
00:01 So, moving on to the first of these diseases, pulmonary emboli. These are blood clots occluding the pulmonary arterial circulation- they are very common, 1 per 1000 per year and, where they come from is, generally speaking, the distal deep leg veins. So, somebody has a deep vein thrombosis with a clot in one of their leg veins, then that clot can break off, move up the vein, venous circulation, reach the right side of the heart and then gets fired into the lung, whereas the pulmonary arteries could get smaller, it will eventually lodge and cause damage distal to where it's lodged. You can also get clots moving it from the arm veins and the right atrium itself, but those are usually associated with indwelling lines. So the patient who has had a long-term catheter in for intravenous antibiotics or has cystic fibrosis for example or perhaps they got a pacing wire or something similar, which allows a clot to form in a place where normally they do not form. 01:05 There are some rare causes of pulmonary emboli, where the material that is embolized to the lung may not actually be clots, and these amniotic fluid embolism which occurs during delivery of a baby, fat embolism which occurs in patients who have had long bone fractures after a motorcycle accident for example, tumor embolism that occasionally occurs where a tumor may actually cause lumps of cancer to fall off into the circulation and fly around to the lungs, and the same thing can happen with infected clots, which it most often occurs in patients who've had intravenous drug abuse, when they have right side endocarditis, and small bits of infected material can fall off the infected valve and go into the lungs to cause clots and abscesses there. And sickle-cell disease is often associated with pulmonary emboli or disease that's similar to pulmonary emboli. 01:58 Deep vein thrombosis and pulmonary emboli have the same risk factors, because deep vein thrombi are the source for pulmonary emboli most of the time. And these risk factors can be divided into three different categories- one is increased coagulation of the blood and the commonest cause of that would be pregnancy, the oral contraceptive pill or other hormonal therapy and malignancy but also occurs when patients have congestive cardiac failure, if they have an increased platelet count due to problems with myeloproliferative disorders of their marrow, in patients with chronic inflammation, and also in smoking. 02:31 Endothelial wall damage will make a clot more likely to occur and this is most obvious in patients who've had pelvic surgery of some description, either gynecological or orthopedic surgery, in which case they have a very high risk of developing a DVT and then potentially a PE after that. And then if the blood flow is reduced because of immobility, surgery, pregnancy, etc. that also make a clot more likely to form. And so, from this you can identify the patients who are most at risk of DVT's and therefore of PEs, and those are patients with malignancy, recent surgery especially pelvic or orthopedic, those who are pregnant, those who've been immobile, due to a long flight or a long car journey etc. 03:16 Emboli to the lungs will vary in their clinical presentation depending on the size of the embolus. And we can divide these into three main categories. In the acute presentation this might be a medium-sized clot, and this will fly off into the pulmonary circulation, but not lodged at the beginning of the pulmonary artery but deeper down in one the medium pulmonary arteries and causing infarction of tissue distal to that. And these patients present with a short history largely of cough, breathlessness, hemoptysis. 03:50 A large clot, large enough to block a pulmonary artery will have a very sudden history, and the main problem these patients will present with is the cardiovascular disturbance from blocking the pulmonary artery. The whole of the body's circulation goes through the pulmonary arteries and therefore if you make a significant obstruction to that, then that's going to have very marked effects on your blood pressure and your cardiovascular function. 04:15 The last presentation is much more chronic, and those are multiple small clots and these patients have a long history which may be developing over weeks or months, and this is due to small emboli clogging off individually a small artery but, which in itself probably has little effect, but when you have multiple emboli clogging off multiple arteries then that eventually will lead to breathlessness, problems with gas exchange, and the patient will present with breathlessness and potentially the consequence of pulmonary hypertension developing due to loss of the arterial circulation due to multiple small clots. 04:54 So the acute presentation, any age, either sex equally, there is usually an obvious pre-existing risk factor, recent surgery, have just been back from Australia, is on the oral contraceptive pill for example. The type of presentation, well the very large clots, that may be cardiac arrest, the patient may just drop dead, essentially. A sudden onset clot not quite enough to stop the heart or cause hypotension, cardiovascular shock, significant respiratory distress. 05:25 The smaller clots, the medium-sized ones, they will cause infarction of the lung and that causes pleuritic inflammation and therefore pleurisy, and pleuritic chest pain, hemoptysis and breathlessness. Those are the classical presentations of somebody with acute PEs. 05:41 With acute PE, the general signs will show that there has been some form of physiological disturbance, there'll be tachycardia, then maybe a 3rd heart sound, raised JVP showing that there's some sort of right heart strain, and of course there might be evidence of the pre-existing DVT, although in many patients that is not clinically apparent. And then there are the respiratory symptoms and signs, they have a raised respiratory rate, there may be a pleural rub over the affected area where the infarction has occurred, and there might be signs of a small effusion which is often associated with that pleural inflammation.
About the Lecture
The lecture Pulmonary Emboli by Jeremy Brown, PhD, MRCP(UK), MBBS is from the course Pulmonary Vascular Disease.
Included Quiz Questions
Which of the following may cause a pulmonary fat embolism?
- Fracture of a long bone
- Atherosclerosis of the carotid artery
- Postpartum hemorrhage
- IV drug abuse
- Penetrating trauma
Which of the following is NOT a risk factor for pulmonary embolism?
- Alcoholism
- Long airplane flight
- Oral contraceptive use
- Indwelling vascular catheter
- Antiphospholipid syndrome
Which of the following is NOT a predisposing factor to pulmonary emboli?
- Decreased elasticity of the vessel wall
- Hypercoagulable state
- Endothelial wall damage
- Stasis in venous blood flow
- Increased viscosity of blood
Author of lecture Pulmonary Emboli

Jeremy Brown, PhD, MRCP(UK), MBBS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Really clear and systematic way of presenting information, I appreciate it alot
