Playlist
Show Playlist
Hide Playlist
Arterial Supply of the Spinal Cord

-
Slides 5 SpinalCord3 BrainAndNervousSystem.pdf
-
Download Lecture Overview
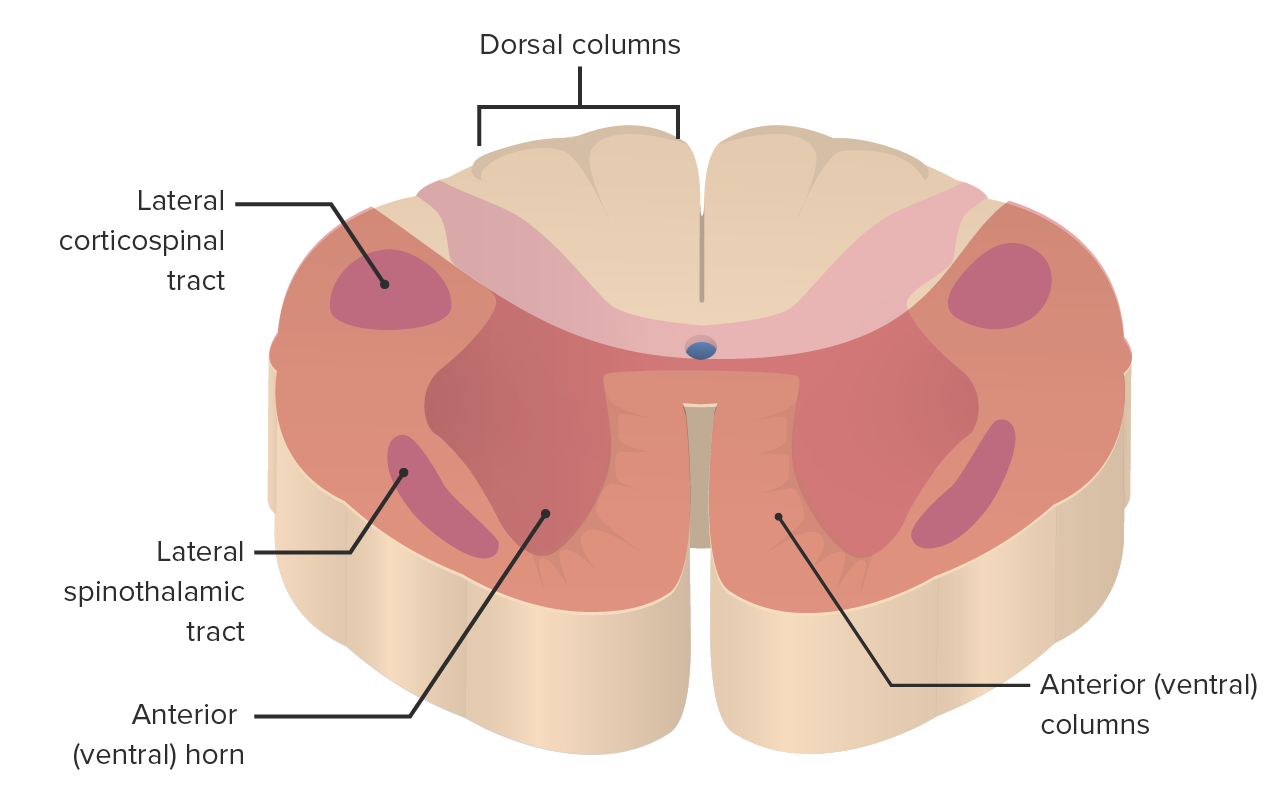
00:00 Here, we’re looking at the arterial supply of the spinal cord. It’s important for you to realize that the spinal cord is supplied by blood vessels that have vertical orientation and horizontal orientation. If we look at the vertical and horizontal sources of the blood supply to the cord, a vertical source is shown here as the anterior spinal artery running on the anterior aspect of your spinal cord. This is a single artery. On the posterior aspect of the spinal cord, you’ll have two spinal arteries. These are the posterior spinal arteries. Collectively, these are responsible for supplying the proximal two-thirds of the spinal cord. This vertical supply is going to be reinforced by horizontal sources. 01:08 These are eight to ten segmental arteries that reinforce the anterior and posterior spinal arteries. Then, the distal part of the spinal cord that’s not very well-supplied by the anterior and posterior spinal arteries is going to be supplied by the largest segmental artery. This is the artery of Adamkiewicz. It is shown down in through here coming in to help supply the distal one-third of the spinal cord. In a repair of abdominal aortic aneurysm, the artery of Adamkiewicz must be considered. If the aorta is cross-clamped proximal to its source of origin, then there can be deficient blood flow to the spinal cord during this surgical operation. As a result, there may be injury to the distal part of the spinal cord as a complication during patient recovery. Now, in consideration of the arterial supply to the spinal cord, I want you to understand an occlusion of one of the blood vessels that supplies the cord. This is going to be anterior spinal artery occlusion. The area shown here is the area of the spinal cord that’s lesioned. What would be the accompanying loss of function as well as some of the features of this disorder? It’s important for you to understand first that anterior spinal artery occlusion is the commonest form of infarction of the spinal cord. As you can see in the area that remains unshaded, back in through here for example, the dorsal columns are uninvolved. They’re spared. So the individual still has preservation of fine touch, vibration, conscious proprioception, for example. Loss of function that accompanies this disorder would be due to a loss of function of the spinothalamic tracts, the corticospinal tracts. This is going to be bilateral. As you can see, this is a bilateral lesion to the spinal cord. There’ll be a loss of pain and temperature below the level of the lesion due to involvement of the spinothalamic tracts. Then, you’ll have a loss of motor function below the level of the lesion due to loss of function of the corticospinal tracts.
About the Lecture
The lecture Arterial Supply of the Spinal Cord by Craig Canby, PhD is from the course Spinal Cord. It contains the following chapters:
- Arterial Supply
- Arterial Spinal Artery Occlusion
Included Quiz Questions
What part of the spinal cord is supplied by the posterior spinal arteries?
- Posterior one-third of the spinal cord
- Distal two-thirds of the spinal cord
- Lateral one-third of the spinal cord
- Anterior one-third of the spinal cord
Which of the following is NOT a feature of anterior spinal artery occlusion?
- Loss of sensation of fine touch and vibration below the level of the lesion
- Loss of temperature sensation below the level of the lesion
- Loss of crude touch sensation below the level of the lesion
- Loss of motor function below the level of the lesion
- Loss of pain sensation below the level of the lesion
Author of lecture Arterial Supply of the Spinal Cord

Craig Canby, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
4 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
This lecture has solved all my problems about spinal cord.
I would recommend this lecture to the osteopathic students snd colleagues
Very nice and clear explanations. Dr. Canby takes a very complicated topic and makes it easy to understand and remember. Thank you!
really nice ,lecture and also good questions at the end to assess,thank you
