Playlist
Show Playlist
Hide Playlist
Constipation in Children: Diagnosis & Management

-
Slides Constipation Pediatrics.pdf
-
Download Lecture Overview
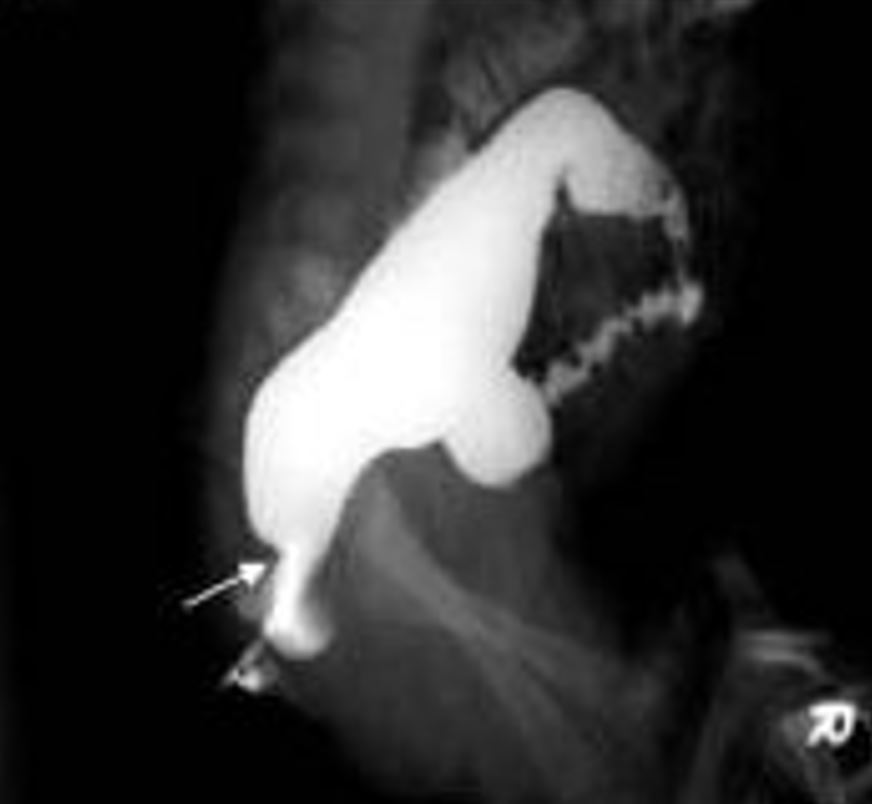
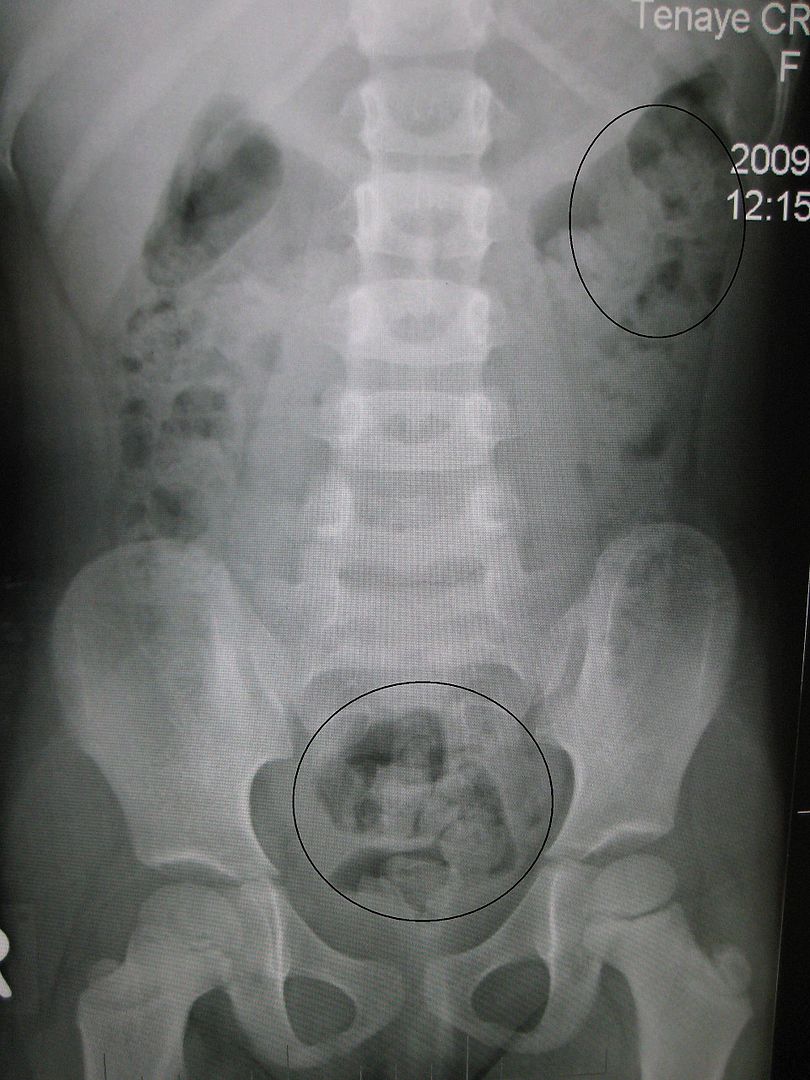
00:02 So most children with constipation do not require diagnostic testing. 00:08 In most cases, if you do a good physical exam and take an excellent history, you can arrive at the diagnosis. 00:14 But there may be cases where you suspect an organic cause. 00:19 For example if a patient has other sequelae of hypothyroidism, we will want to check to see if that’s the cause of the constipation. 00:26 So examples of some labs we might get are electrolytes, thyroid functions, lead levels, lead toxicity can cause constipation, or sweat testing. 00:35 Again, testing for cystic fibrosis. 00:39 You can, if you are concerned or confused as to whether a child is constipated, obtain an abdominal X-ray, but be careful. 00:46 Abdominal X-rays have both a false negative and a false positive rate. 00:51 The history is much better than the X-ray. 00:55 In cases where a child is having problem defecating that are very severe, we may suspect a problem with the actual enervation of the rectal tissue. 01:06 In this case, a rectal biopsy may be in order, in order to look for ganglion cells within that rectal tissue to see if this patient has Hirschsprung’s disease. 01:16 We may also do things like manometry where we measure the pressure when the rectal sphincter is dilated and we may do something like a barium enema to look at the contour of the inner surface of the mucosa. 01:31 Lastly, we may get spinal X-rays or MRIs if we’re concerned for some sort of spinal abnormality or neurologic impairment. 01:39 And I’ve never done this, but one could certainly do it, which is a colon transit study for patients who failed to respond to aggressive treatment in case you’re wondering whether there’s some functional problem with the colon. 01:53 So how do we treat constipation? Most of it’s functional. 01:57 In infants under one year of age, we’ll generally start with something as simple as glycerin suppositories. 02:03 Even before that, we might just suggest to the mother to use the rectal thermometer to stimulate the rectal area a little bit and sometimes that’s all that’s needed to get a kid to go. 02:14 On the other hand, we may use osmotically active carbohydrates. 02:18 An example would be prune juice in a very young child and that osmotic juice will go all the way through the colon and cause fluid to come into the colon, thereby loosening up the stool and improving the problem. 02:34 Lastly, you can use osmotic laxatives like propylene glycol, which is act in the same way. 02:42 In older children, we may do enemas to relieve that distal obstruction before we apply a medicine that will chronically loosen up the stools. 02:53 We can also do Bisacodyl suppositories for these children to try and get things going from the backend. 02:59 If they’re truly obstructed, we’re going to do something from the front end such as oral or NG polyethylene glycol. 03:08 NG polyethylene glycol is really what we reserve for those very severely constipated children where we simply can’t clean them out well enough. 03:18 These children, we’ll apply an NG tube and put in remarkably high rates of polyethylene glycol, in up to four liters over several hours. 03:30 This acts like Roto-Reuter. 03:32 It drives right through and everything comes out. 03:35 And you stop when they’re pooping clear NG-administered polyethylene glycol. 03:42 You can also do a manual disimpaction and this is sometimes important for children where you simply can’t get the hard stool out the other end. 03:51 What’s most important for constipation, however, is prevention. 03:56 One way you can prevent it from ever starting is encourage breastfeeding. 04:01 Babies who are breastfed stool very frequent and are almost never constipated. 04:05 However, in older children, you would recommend a balanced diet. 04:10 Whole grain, fruits and vegetables. 04:13 The idea is to optimize the fiber and that’s a good habit to get into because lifelong fiber administration prevents things like colon cancer. 04:23 For children who are still having problems, we will advance to adding osmotic laxatives like polyethylene glycol or what we call Miralax powder, which you can provide to the child. 04:34 Because this comes as a powder and can be easily admixed with the beverage of your choice, children are capable of finding the dose that works for them. 04:43 Too much, they get diarrhea. 04:44 Too little, they’re constipated. 04:46 Generally, families figure out what dose is right for that child. 04:51 There are stimulants that can help in the acute setting such as senna, but we don’t like to use stimulants regularly because they can become addictive and that you need your stimulant in order to stool. 05:04 So we don’t typically start with those. 05:07 And most importantly, parental education. 05:10 Avoid reprimanding and punishing children around the toileting behavior that they’re having. 05:16 We do after we clean the child out with some NG GoLYTELY or polyethylene glycol, we will frequently encourage behavior modification in children who are old enough to be using the toilet. 05:29 We’ll recommend regular toilet sitting twice a day for half hour even if they don’t have to go. 05:34 Remember, they may have to go even though they don’t sense it because of that dilated rectal vault. 05:40 We recommend parents to do stool diaries and engage in a reward system such as candy, which will allow the families to reward children for a job well done.
About the Lecture
The lecture Constipation in Children: Diagnosis & Management by Brian Alverson, MD is from the course Pediatric Gastroenterology.
Included Quiz Questions
Which is NOT a maintenance therapy for constipation?
- Senna
- Osmotic laxatives
- Fiber in the diet
- Regular toileting
- Positive reinforcement training
Which of the following tests is least likely to show abnormal findings in the workup of an infant with chronic constipation?
- Stool for ova and parasites
- Serum electrolytes
- Thyroid function tests
- Lead levels
- Sweat chloride levels
Which of the following is the most appropriate next step in treating a 10-month-old child with recent onset constipation in whom dietary modification and rectal stimulation has not been effective?
- Glycerin suppositories
- Propylene glycol
- Prune juice
- Barium enemas
- Bisacodyl suppositories
Author of lecture Constipation in Children: Diagnosis & Management

Brian Alverson, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Good lecture, very useful to know how constipation is treated in the US. There are some differences with my local recommendations (Europe).
