Playlist
Show Playlist
Hide Playlist
Type I Membranoproliferative Glomerulonephritis (MPGN)



-
Slides MembranoproliferativeGlomerulonephritis RenalPathology.pdf
-
Download Lecture Overview
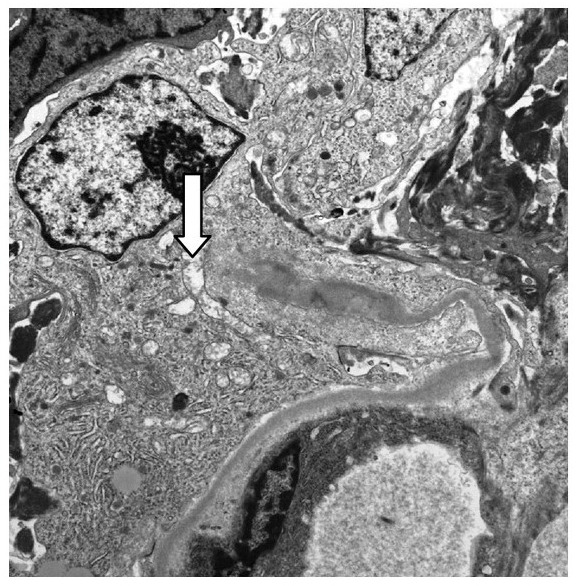
00:00 Type I MPGN. Most common type it is. 00:03 Nephrotic syndrome presentation, what does that mean to you? You begin with protein loss. 00:09 And greater than 3.5 grams of protein per day. 00:11 Hypoalbuminemia and generalized edema. 00:15 You would have loss of antithrombin III, Anticoagulation, maybe a little bit of hypertension. 00:20 That's your nephrotic presentation, isn't it? Some cases it will have nephritic. 00:25 I told you earlier that MPGN and DPGN will have a little bit of nephritic, a little bit of nephrotic. 00:33 Now, most of this with MPGN in fact, is nephrotic. 00:36 Associated with hepatitis C, more common or cryoglobulinemia. 00:42 What does that even mean? That means that you might have conditions and at some point in time, when you get into cryoglobulinemia, there are three different types. 00:51 One, two, and three, cryoglobulinemia. 00:52 The big ones. 00:53 Type I associated with multi-myeloma. 00:57 Type II and III, more or less associated with infections and autoimmune diseases. 01:02 What do all of these have in common? Autoimmune diseases. 01:05 Monoclonal gammopathies and hepatitis C could be put in there as well. 01:10 They are associated with antigen-antibody complexes. Okay. 01:19 Two components, circulating through the body. 01:23 All of a sudden cryo. 01:24 What does that mean? Cold exposure. 01:29 The globulins will precipitate resulting in all kinds of issues in your patient. 01:34 Mostly, what do you know this about Waldenstrom? In Waldenstrom, what then happens when you have your globulins that will precipitate in the blood? It’s almost like a thrombus, isn't it? And so therefore it’s hyperviscosity. Hyperviscosity. 01:52 Cryoglobulinemia is a big deal, a big clinical condition or syndrome, and I've given you a few examples of type I, type II, type III. 02:01 My point at this point though, what kind of MPGN are we dealing with? Type I. 02:07 In the previous discussion what branch of our MPGN would that follow? Immunecomplex mediated or would it be complement-mediated? Good, immune complex mediated. Much more common, type I. 02:23 Which type I? On your light microscopy, can't really tell the difference between type I and type II, that I can tell you for certain. 02:31 However, where you can start seeing differences? When you hear at this point, it should be reflexive. 02:39 When you say subendothelial immune complexes, what kind of biopsy is this? Good. Electron microscopy. 02:46 If you see a granular pattern, what kind of biopsy is that? Good. Immunofluorescence. 02:51 Aren’t you feeling good about this now? You're reading, as if you’re reading a clinical vignette. 02:55 You're reading as if it was a medical journal. 02:56 Lancet, New England’s Journal Of Medicine. Whatever it may be. 02:59 And these are the kind of information that it has and you should be able to- These are the kind of questions, information that everyone expects you to know, at your level of medical education. 03:11 The immune complexes activate classical and alternative complement pathway. 03:16 You know that already. 03:17 Electron microscopy shows tram-track. 03:22 What’s that even mean? Tram-track means, the membranes being involved, membranoproliferative. 03:28 The membranes been involve, what happens? Split of the glomerular basement membrane by ingrowth of mesangium. 03:37 Tram-track, is that specific? No. It’s not. 03:41 Anything that weakens that membrane, do you think that you would then have deposition of mesangium and splitting of it? Sure. Another good differential, Alport Syndrome. 03:51 Hypertension, 35% of the majority of your patients will have hematuria. 03:56 Remember, MPGN? Nephritic/Nephrotic presentation. 03:59 Majority will progress to chronic renal failure. 04:02 Which was most common, type I or type II? Type I. 04:06 If it’s type I, what kind of association? Immune complexes. 04:10 Examples, autoimmune disease, infections such as Hepatitis C and cryoglobulinemia. 04:17 And we have monoclonal gammopathies, including Waldenstrom. 04:21 With type I, response to corticosteroids not established, let it go.
About the Lecture
The lecture Type I Membranoproliferative Glomerulonephritis (MPGN) by Carlo Raj, MD is from the course Glomerulonephritis.
Included Quiz Questions
The proliferation of what cell type is primarily responsible for the "tram-track" appearance of the membrane in membranoproliferative glomerulopathy?
- Mesangial cells
- Parietal epithelial cells
- Fenestrated cells
- Endothelial cells
- Visceral epithelial cells
Which of the following statements about Type I membranoproliferative glomerulonephritis (MPGN) is correct?
- All statements are correct.
- It most commonly has a nephrotic presentation but may also have a nephritic presentation.
- Immune complexes may activate the classical complement pathway, the alternative complement pathway, or both.
- It may be associated with cryoglobulinemia.
- It is the most common type of MPGN.
Which of the following statements about cryoglobulinemia is CORRECT?
- Large amount of protein usually immunoglobulins that precipitate at reduced temperatures
- Immunoglobulins that cause agglutination of red blood cells
- It is a type of hypoviscosity syndrome.
- It is often associated with bacterial infections.
- It often leads to type II membranoproliferative glomerulonephritis.
Which of the following appearances on electron microscopy is characteristic of type 1 MPGN?
- Tram-track appearance due to GBM splitting caused by mesangial ingrowth
- Mesangial immune complex deposits
- Subepithelial immune complex humps
- Effacement of foot processes
- Spike and dome appearance with subepithelial deposits
Which of the following clinical manifestations can be present in type 1 MPGN?
- Hypertension
- Hypotension
- Polyuria
- WBC casts in the urine
- Granular casts in the urine
Author of lecture Type I Membranoproliferative Glomerulonephritis (MPGN)

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
