Playlist
Show Playlist
Hide Playlist
Diffuse Proliferative Glomerulonephritis


-
Slides Glomerulonephritis.pdf
-
Download Lecture Overview
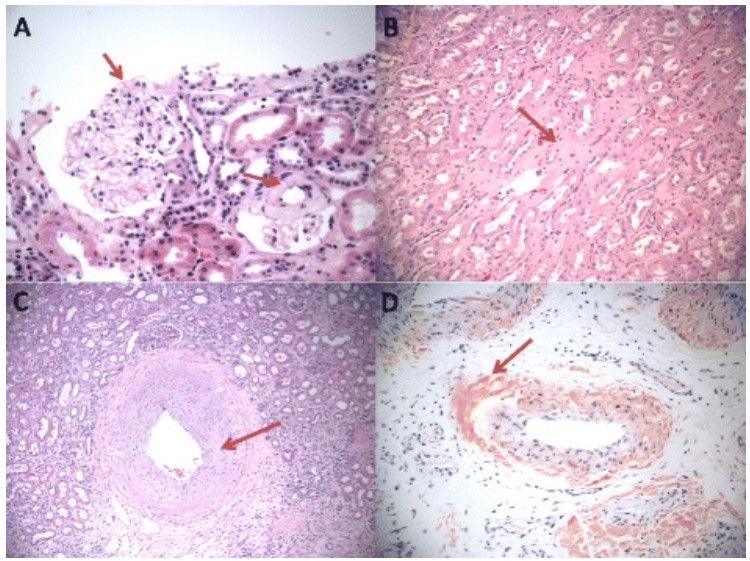
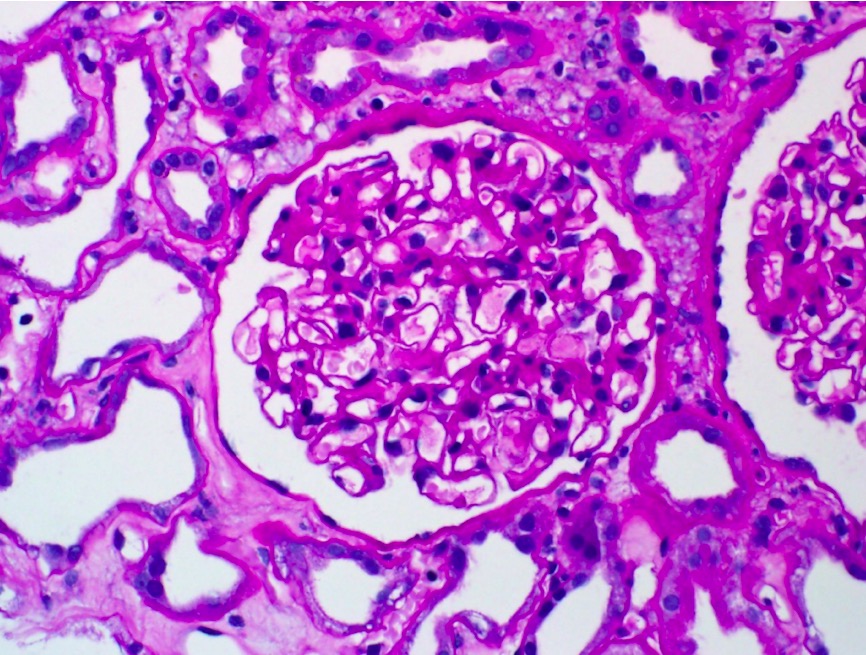
00:01 Now, we're going to our next glomerulonephritis, and this one is an interesting one. 00:06 This is called DPGN. 00:08 The reason I called this interesting is for two main reasons. 00:10 Number one, it’s a fact that really, in terms of your presentation, it will be nephritic, nephrotic, nephritic, nephrotic. 00:18 And by that I mean, oh, well, there might be hematuria and RBC casts that are involved in hypertension. 00:23 But there might be actual protein loss of being greater than 3.5 grams of protein. 00:28 There might be lipid that is then risen. Interesting. 00:31 So I just gave you the symptoms in this patient that has components of both nephritic and nephrotic. 00:37 DPGN will do that. 00:39 Also, the second important point, is that this is the prototype. 00:43 This is the most common subtype of SLE induced kidney damage. 00:48 Now, the other types can have a nephrotic presentation but what you're keeping in mind is if your patient has SLE and comes back to be positive for anti-double stranded DNA, the most likely type of kidney damage or glomerulonephritis that you're finding in this patient is going to be DPGN. 01:06 Now, what you have to memorize is DPGN, will be sub-endothelial. 01:13 Earlier with P, PSGN, it was sub-epithelial. 01:19 With DPGN, it’s sub-endothelial. Are we clear? Now, I don’t care how you do it, you memorize that. 01:28 This immune-complex that’s being deposited, where are you? On the side of the blood and the capillary lumen or are you on the side of your urine and your podocyte? Sub-endothelial, will be underneath your endothelial cell in the capillary lumen between the endothelial cell and the basement membrane. 01:46 With that said, if you find such a deposition, on electron microscopy, what are you going to find in immunofluorescence? You tell me the description. Very good. It's a granular. 01:56 Next, if you find this to be SLE induced then, what is this called? A DNA, anti-DNA immunocomplexes or in other words, Anti-double stranded DNA. 02:07 You're also going to find activation of your complement pathway but any immune-complex will do that. 02:13 Now, what you do find, and the description is called wire looping of the capillaries corresponding to sub-endothelial immune-complex. 02:21 There’s going to be neutrophil infiltration with hyaline thrombi in the capillary lumen. 02:26 There’s enough information here for you to properly diagnose your patient with DPGN. 02:30 Look for SLE and look for anti-double stranded DNA, and the fact that you have sub-endothelial deposits giving you a granular pattern. 02:38 Next, kidneys are major target organ in SLE for DPGN. 02:44 Your serum ANA test usually has a rim pattern which then corresponds with, please take a look, anti-double stranded DNA. 02:54 How many kidneys do you have? Two. Double stranded. 02:57 If it’s SLE in antihistone, it’s drug induced SLE, isn't it? And by drug-induced, you might be thinking about, well, procainamide. 03:07 You might be thinking about hydralazine, isoniazid, and for different reasons, maybe phenytoin. 03:14 Evolves into chronic renal failure in most cases. 03:18 And ends up being a common cause of death in a patient with SLE is actually chronic renal failure. 03:26 An important point. 03:28 Please make sure that you're quite familiar with the SLE induced DPGN issue resulting to chronic renal failure with the various tests that we just walked through.
About the Lecture
The lecture Diffuse Proliferative Glomerulonephritis by Carlo Raj, MD is from the course Glomerulonephritis.
Included Quiz Questions
Which of the following conditions manifests with a combination of nephritic and nephrotic syndromes in systemic lupus erythematosus?
- Diffuse proliferative glomerulonephritis
- IgA nephropathy
- Post-streptococcal glomerulonephritis
- Membranous glomerulonephritis
- Membranoproliferative glomerulonephritis
Which of the following immunocomplex deposition patterns is characteristic of diffuse proliferative glomerulonephritis?
- "Wire looping" of capillaries and subendothelial depositions
- "Wire looping" of capillaries and subepithelial depositions
- "Wire looping" of podocytes and subendothelial depositions
- "Tram tracking" of the basement membrane and subendothelial depositions
- "Wire looping" of the basement membrane and subendothelial depositions
Author of lecture Diffuse Proliferative Glomerulonephritis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
