Playlist
Show Playlist
Hide Playlist
Hirschsprung's Disease (Congenital Megacolon)


-
Slides Constipation Pediatrics.pdf
-
Download Lecture Overview
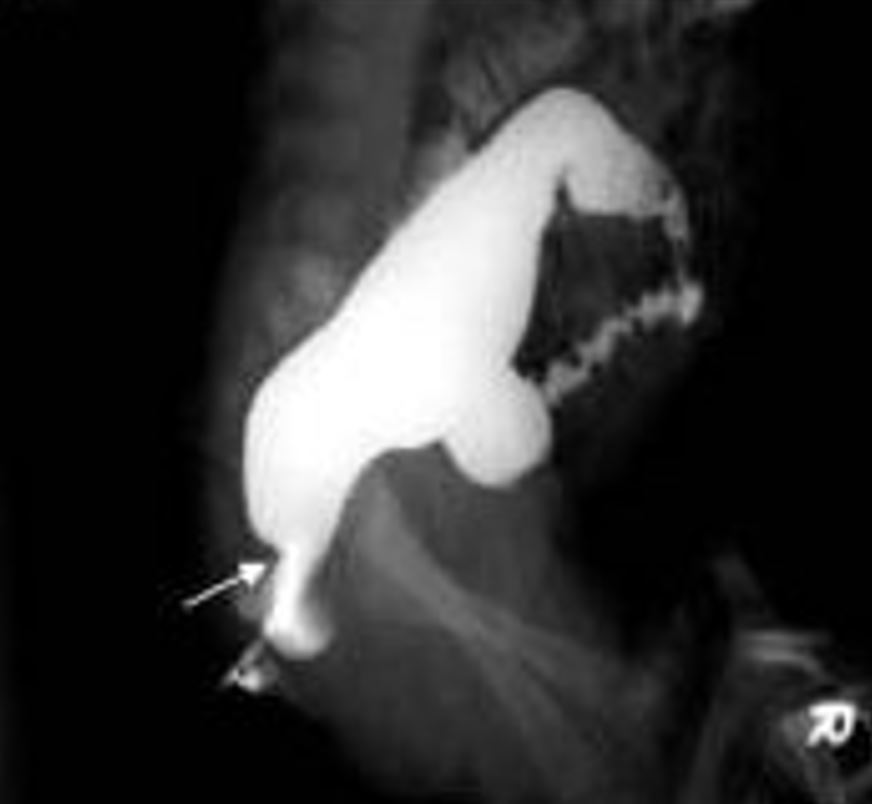
00:02 There are some situations, however, where behavioral modification simply isn’t enough, and this is one of them. 00:10 So this is Hirschsprung’s disease, which is a congenital aganglionic megacolon. 00:16 The problem here is in the mucosa, which you can see here in the slide, the nerves have not successfully entered the smooth muscle and the muscle of the rectal sphincter. 00:29 As a result, they’re having a hard time relaxing the rectal tone. 00:35 Because that rectal tone will not relax, these children simply aren’t capable of defecating, whether they want to or not, and no matter how much fiber is in their diet. 00:47 This is a congenital absence of ganglion cells in the bowel wall. 00:54 So this happens because of a failure of neural crest cell migration from the proximal to the distal bowel. 01:01 It is sporadic. 01:02 It’s not necessarily inherited, it’s just something that happens to happen. 01:06 And this absence of submucosal and myenteric plexus results in an inability to relax the bowel and obstruction. 01:16 It begins at the anus and extends proximally in a continuous manner. 01:21 That is to say that you will notice there’s no skip lesions. 01:26 There are variable amounts of bowel involvement. 01:29 About 80% of children only have the distal end of the rectosigmoid colon involved. 01:34 However, 10% to 15% will have involvement of the entire colon; 5% will have entire bowel involvement. 01:46 So very severe Hirschsprung’s presents typically earlier, and some children present later because they are getting by okay and the parents are just considering their child a very constipated child but it’s not until later that people figure out that this was the problem. 02:03 In neonates, they’ll present generally with a failure to pass meconium. 02:07 Remember that 48-hour rule. 02:09 We really want to see the meconium come by then. 02:12 Another problem that might cause that, remember, is cystic fibrosis. 02:16 These infants or neonates will have distended abdomens, they may have emesis, and they will often have feeding intolerance because they just feel full and don’t want to eat anymore. 02:27 Older infants usually have a history of chronic constipation. 02:30 This is a problem that’s been going on for a long time, and the parents are sometimes frustrated, they can’t figure out what’s going on. 02:38 There’s often dilatation of proximal bowel accommodating this retained fecal material. 02:44 These children may have failure to thrive because they’re not eating as much as they should because of a feeling of satiety and discomfort from their abdomen. 02:53 And remember, children with Hirschsprung’s disease can become septic with a simple viral gastroenteritis. 03:01 While we think of this as a completely benign entity in other children, children with Hirschsprung’s disease, the diarrhea has nowhere to go. 03:10 This causes an intestinal dilatation which can cause bacteria to migrate into the intestinal wall, and those children can go into septic shock, develop peritonitis and get in big trouble. 03:22 We really worry about even viral gastroenteritis in children with Hirschsprung’s disease. 03:31 So, if we suspect Hirschsprung’s disease, what are we going to do? Well, the gold standard is a rectal suction biopsy. 03:39 The surgeon will go in and create some suction on the rectal vault wall and take a biopsy and then we'll look for ganglion cells. 03:48 There won’t be any. 03:49 The problem is that in a normal rectal biopsy, occasionally, you just haven’t happen to find the ganglion cells. 03:58 So this isn’t totally as straightforward as you'd expect. 04:01 You’re always worried that you’re falsely diagnosing someone just because you haven’t found the ganglion cells. 04:07 This becomes a pathologist on a search for something that really isn’t there. 04:12 Sometimes, a contrast enema can tell us some clues. 04:16 We may see a transition zone on the enema between the narrow aganglionic distal bowel, and then proximally, the distended normal bowel before it. 04:29 And if we see a clear transition zone, that may be a clue that this is Hirschsprung’s disease. 04:35 Flipside, and this is unusual but it certainly can be done when we’re still not sure. 04:41 We can dilate the anal sphincter and then measure the pressure with that balloon. 04:48 If the anal sphincter is not relaxing as the rectum is dilated, y you have a sense that there’s a problem with the anal rectal tone because normally, the rectal sphincter should relax as it allows to pass fecal material through it. 05:09 So, what is the treatment of Hirschsprung’s disease? Surgery is the only therapy, and this is a little bit difficult. 05:17 Typically, we resect aganglionic bowel however much there is, and do a pull through of normal bowel for an anastomosis with the anus. 05:30 Sometimes, surgeons can create a little bit of a rectal pouch, but these patients have a hard time stooling for the rest of their life. 05:38 They can have normal bowel function, but sometimes they have to stool more frequently. 05:46 There are potential recurring symptoms. 05:48 First is they may have fecal incontinence from a smaller rectal pouch that has been reconstructed and fecal material can leak through. 05:58 They may have residual constipation if there is remaining aganglionic bowel there. 06:04 And again, the enterocolitis problem can still rear its ugly head for several months after the surgery. 06:11 So, we still worry about gastroenteritis in these children, and if they are treated for gastroenteritis, they may be empirically placed on broad spectrum antibiotics such as Zosyn until they’re feeling better to prevent bacterial invasion into the bowel wall and peritonitis. 06:30 That’s everything I have for you today about constipation and Hirschsprung’s disease. 06:35 Thanks for your attention.
About the Lecture
The lecture Hirschsprung's Disease (Congenital Megacolon) by Brian Alverson, MD is from the course Pediatric Gastroenterology.
Included Quiz Questions
A patient with Hirschsprung's disease presents with gastroenteritis. Which of the following may be indicated?
- Broad-spectrum antibiotics
- Immodium
- NG polyethylene glycol
- Nonsteroidal anti-inflammatory drug
- Regular toileting
The pathology in Hirschsprung's disease is a failure of ganglion cells to migrate into the muscular layers of the rectal wall leading to which of the following?
- Failure of the rectal sphincter to relax
- Failure of the rectal sphincter to constrict
- Failure of formation of rectal valves
- Failure of complete rectal wall formation
- Failure of formation of the entire muscular wall of rectum
A patient with Hirschprung's disease undergoes rectal biopsy. In addition, a contrast enema is also performed which shows a transition zone. Which of the following is true about the transition zone?
- It is formed in between narrow aganglionic distal bowel and distended normal bowel proximal to it
- It is formed in between the distended aganglionic distal bowel and narrow normal bowel proximal to it
- The transition zone is a normal variant
- The transition zone is highly suggestive of absence of Hirschprung's disease
- It is formed in between rectum and sigmoid colon
What is the most common etiology of Hirschsprung's disease (congenital megacolon)?
- Sporadic
- Diet-related
- Hereditary
- Infectious
- Endemic
Author of lecture Hirschsprung's Disease (Congenital Megacolon)

Brian Alverson, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Good lecture, all aspects of the diseases are explained in a clear manner.
